
0 CORPORATE OVERVIEW June 2024 Issuer Free Writing Prospectus dated June 21 , 2024 Filed Pursuant to Rule 433 of the Securities Act 1933 , as amended Relating to Preliminary Prospectus dated June 21 , 2024 Registration Statement No . 333 - 279734

1 Legal Disclaimer Actuate Therapeutics, Inc. (the "Company," "Actuate," "we," "our" and "us") has filed a registration statement (including a p rel iminary prospectus) on Form S - 1 (File No. 333 - 279734) related to this proposed initial public offering with the Securities and Exchange Commission (the "SE C"). The registration statement has not yet become effective. Shares of our common stock may not be sold, nor may offers to buy be accepted, prior to the registration statement becoming effective. Before you invest, you should read the preliminary prospectus in that registration statement, an d when available, the final prospectus relating to the offering, and the other documents we have filed with the SEC for more complete information a bou t us and the proposed offering. You may get these documents for free by visiting EDGAR on the SEC website at ww.sec.gov. Alternatively, a copy of th e prospectus may be obtained from Titan Partners Group LLC, a division of American Capital Partners, LLC at 4 World Trade Center, 29th Floor, Ne w Y ork, NY 10007, by phone at (929) 833 - 1246 or by email at prospectus@titanpartnersgrp.com. This presentation shall not constitute an offer to sell or the solicitation of an offer to buy any securities, nor shall ther e b e any sale of these securities in any state or jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification und er the securities laws of any such state or jurisdiction. Sales and offers to sell our securities will only be made in accordance with the Securities Act o f 1 933, as amended, and applicable SEC regulations, including written prospectus requirements.

2 Forward - Looking Statements This presentation contains forward - looking statements. Forward - looking statements are not historical facts but are based on cert ain assumptions of our management, which we believe to be reasonable but are inherently uncertain, and describe our future plans, strategies and exp ect ations. Forward - looking statements can generally be identified by the use of forward - looking terminology, including, but not limited to, “may,” “could,” “seek,” “guidance,” “predict,” “potential,” “likely,” “believe,” “will,” “expect,” “anticipate,” “estimate,” “plan,” “intend,” “forecast,” or variations of these terms a nd similar expressions, or the negative of these terms or similar expressions. Past performance is not a guarantee of future results or returns and no representation or warranty is ma de regarding future performance. These statements relate to future events and involve known and unknown risks, uncertainties and other important factors beyon d o ur control which may cause our actual results, performance or achievements to be materially different from any future performances or achievements expressed or implied by the forward - looking statements. Each of these statements is based only on current information, assumptions and expectations that are inherently s ubj ect to change and involve a number of risks and uncertainties. Such statements include, but are not limited to, statements about: expectations regarding our capitalization and resources; the adequacy of our capital to support our future operations and our ability to successfully initiate and complete pre - clinical and clinical trials; our strategy and focus; the research, development and commercial potential of any of our product candidates; the timing and success of our development ef for ts; the success of any of our planned preclinical and clinical trials and our ability to achieve regulatory approval for elraglusib or any future product candidate; the potential benefit of, and ability to enter into, modify, or terminate collaborative agreements; the timing and likelihood of regulatory filings with the FDA; the ant icipated timing, costs, design and conduct of our ongoing and planned clinical trials and preclinical studies for elraglusib and any future product candidates; our ability to commercialize elraglusib and any future product candidates, if approved; the pricing and reimbursement of elraglusib and any future product candidates, if approved; the potential to develop future product candidates; the potential market or success for the clinical development programs of Actuate; and statements o f h istorical fact, including those related to Actuate’s future cash, market or financial position. Actuate may not actually achieve the plans, carry out the intentions or meet the expectations or projections disclosed in any fo rward - looking statements such as the foregoing, and you should not place undue reliance on such forward - looking statements. The forward - looking statements contained or implied in this presentation are subject to other risks and uncertainties. Except as otherwise required by law, we disclaim any intention or obligation to up date or revise any forward - looking statements, which speak only as of the date they were made, whether as a result of new information, future events or circumst anc es or otherwise. The products and claims made about specific products in this presentation have not been evaluated by the United States Food and Drug Administr ati on or any foreign equivalent and are not approved to diagnose, treat, cure or prevent disease.

3 Transaction Overview Actuate Therapeutics, Inc. (Nasdaq: ACTU) Initial Public Offering $50.0 million (+15% Over - allotment Option) 5,555,556 Shares of Common Stock $8.00 - $10.00 per Share For clinical trials and product development, research and development, clinical manufacturing as well as for working capital and other general corporate purposes Titan Partners Group, a division of American Capital Partners Newbridge Securities Corporation

4 Company Highlights 1 Developing elraglusib , a leading GSK - 3 β inhibitor with novel, multimodal MOA, in multiple advanced cancer Phase 2 trials 4 Oral version of elraglusib successfully evaluated in Healthy Volunteer Phase 1 ▶ Phase 1 dose escalation study planned in advanced cancer patients in 2H 2024 ▶ Potentially expands clinical and commercial opportunities 3 Extended survival and increased responses are observed in mPDAC and relapsed/ refractory Ewing sarcoma. Preliminary evidence of clinical benefit has also been observed in patients with metastatic melanoma and relapsed/refractory colorectal and lung cancer, which will be used to inform prioritization of the near - term pipeline 5 Broad composition of matter IP protection and development incentives ▶ Orphan Drug and Fast Track Designations for pancreatic or other cancer types could accelerate path to registration 2 Clinical responses (CRs/PRs) and Disease Control observed across cancer histologies with elraglusib IV as single agent and in combination with chemotherapy

5 • Elraglusib is an ATP - competitive inhibitor of GSK - 3 β • GSK - 3 β has been shown to potentially contribute to tumor progression in many treatment naive and refractory/resistant tumors • Pleiotropic effects as signaling adaptor • Elraglusib downregulates well - credentialed molecular pathways that can lead to chemotherapy and drug resistance • NF - kB pathway - anti - apoptotic protein expression • Alterations in TGF - b and pro - inflammatory cytokines suggest role in fibrosis in addition to immunomodulation • DDR pathways (ATR/ATM) including mismatch repair (PMS2) • Increase responsiveness of resistant/refractory tumors to chemo and immune therapy - ”cold” tumors turned to “hot” • Inhibition of oncogenic epithelial - mesenchymal transitions Source: Molecular Pathways , 2017; DOI: 10.1158/1078 - 0432.CCR - 15 - 2240. Multimodal MOA Supported by Clinical Data

6 Note: As of May 202 4 Multimodal MOA Supported by Clinical Data Elraglusib Injection Elraglusib Oral Tablet Pediatric Adult Actuate - 1801 Pediatric Actuate - 1902 Adult Actuate - 2401 Part 3B: Pancreatic Cancer (combined with GnP ) 1st line metastatic (randomized, controlled) Fast track designation Part 1 and 2: Dose Escalation Refractory Cancers Part 3A: Pancreatic Cancer (combined with GnP ) 1st line metastatic (single arm) Phase 2 Study Amendment in development for Ewing Sarcoma Only Phase 1 / 2: Ewing Sarcoma Patients Only Phase 2: • Melanoma (metastatic, CPI refractory) • Colorectal cancer (metastatic, refractory) Phase 1: Advanced, refractory solid cancers Phase 1: Advanced, refractory cancer (solid and hematological) Published Carneiro et al. 2024 Submitted for publication Topline Data: Q1 2025 Topline Data: 2H 2025 FPFD: 2H 2024 RP2D: 1H 2025 Topline Data: 1H 2026 TBD Study Phase 1 Phase 2 Phase 3 Anticipated Milestones Fully Enrolled Completed Fully Enrolled Ongoing In Planning In Planning In Planning GnP : gemcitabine/nab - paclitaxel FPFD: First patient first dose RP2D: Recommended Phase 2 Dose Drug Within each study (1801, 1902, 2401), each subsequent part or phase is successive to the preceding part or phase and not a separate study that will individually proceed through each of phases 1, 2, and 3 of clinical trials.

7 Establishes process for transition from elraglusib (9 - ING - 41) Monotherapy (Part 1) to evaluation of multiple chemotherapy combinations (Part 2) to Phase 2 efficacy studies (Part 3) under one protocol Elraglusib + Gemcitabine Elraglusib + Doxorubicin Elraglusib + Carboplatin Elraglusib + Lomustine Elraglusib + Irinotecan Elraglusib + GnP Elraglusib + Paclitaxel Carboplatin Elraglusib + Pemetrexed Carboplatin 1801 - Part 3 Company Sponsored Phase 2 Studies 1801 - Part 3B First line mPDAC GnP + elraglusib Randomized Controlled Trial (International) Utilize rationale from Actuate - 1801 to identify indications for Phase 2 studies with elraglusib oral tablet Clinical Study Actuate - 1801 1801 - Part 2 Elraglusib Dose Escalation in Combination with Standard Dosing Chemotherapy All patients required to have previously failed the combination chemo prior to enrollment 1801 - Part 1 Elraglusib Monotherapy Dose Escalation 1801 - Part 3A First Line mPDAC GnP + elraglusib Simon Two - Stage (International) Phase 1/2 Study Design for Elraglusib Injection GnP : gemcitabine/nab - paclitaxel

8 As Monotherapy and in combination with chemotherapy Treatment - Emergent Adverse Events of Any Grade Reported in 20% of Patients Treated with elraglusib in Actuate 1801 Part 1 and 2 Treatment - Emergent Adverse Events of Any Grade Reported in 20% of Patients Treated with elraglusib (December 31, 2023) in Actuate 1801 Part 3B (ongoing) Patients, n (%) Patients, n (%) Adverse event Elraglusib monotherapy Part 1 (N=67) Elraglusib with chemotherapy Part 2 (N=171) Adverse event Elraglusib with Nab - Paclitaxel + Gemcitabine (N=139) Nab - Paclitaxel + Gemcitabine (N=62) Any Grade Grade 3 Any Grade Grade 3 Any Grade Grade ≥3 Any Grade Grade ≥3 Any TEAE 67 (100) 37 (55.2) 171 (100) 124 (72.5) Any TEAE 128 (92.1) 105 (75.5) 54 (87.1) 33 (53.2) Serious TEAE 29 (43.3) 26 (38.8) 72 (42.1) 67 (39.2) Serious TEAE 63 (45.3) 60 (43.2) 25 (40.3) 23 (37.1) Leading to treatment discontinuation 6 (9) 4 (6) 36 (21.1) 30 (17.5) Leading to Stoppage of Any Study Drug 19 (13.7) 16 (11.5) 8 (12.9) 8 (12.9) Leading to death 5 (7.5) 5 (7.5) 18 (10.5) 18 (10.5) Leading to death 13 (9.4) 13 (9.4) 8 (12.9) 8 (12.9) TEAEs of any Grade in 20% of Patients TEAEs of any Grade in 20% of Patients Visual impairment 34 (50.7) 0 104 (60.8) 1 (0.6) Visual impairment 80 (57.6) 0 3 (4.8) 0 Fatigue 32 (47.8) 2 (3) 86 (50.3) 8 (4.7) Neutropenia 1 67 (48.2) 63 (45.3) 17 (27.4) 11 (17.7) Nausea 25 (37.3) 1 (1.5) 77 (45) 3 (1.8) Fatigue 64 (46) 15 (10.8) 18 (29) 1 (1.6) Diarrhea 21 (31.3) 3 (4.5) 52 (30.4) 6 (3.5) Nausea 61 (43.9) 10 (7.2) 19 (30.6) 1 (1.6) Anemia 17 (25.4) 4 (6) 80 (46.8) 43 (25.2) Diarrhea 57 (41) 11 (7.9) 19 (30.6) 2 (3.2) Vomiting 17 (25.4) 1 (1.5) 47 (27.5) 5 (2.9) Anemia 2 45 (32.4) 25 (18) 14 (22.6) 8 (12.9) Headache 16 (23.9) 0 36 (21.1) 1 (0.6) Alopecia 43 (30.9) 1 (0.7) 18 (29) 0 Abdominal pain 12 (17.9) 3 (4.5) 38 (22.2) 6 (3.5) Decreased appetite 41 (29.5) 5 (3.6) 9 (14.5) 2 (3.2) Neutrophil count decrease 2 (3) 2 (3) 45 (26.3) 36 (21.1) Thrombocytopenia 3 38 (27.3) 11 (7.9) 12 (19.4) 2 (3.2) Platelet count decrease 1 (1.5) 0 50 (29.2) 27 (15.8) Vomiting 36 (25.9) 2 (1.4) 15 (24.2) 1 (1.6) White blood cell count decrease Not reported Not reported 42 (24.6) 28 (16.3) Constipation 36 (25.9) 2 (1.4) 14 (22.6) 1 (1.6) 1. Includes PT terms neutropenia and neutrophil count decreased 2. Includes PT terms anemia and hemoglobin decreased 3. Includes PT terms thrombocytopenia and platelet count decreased Safety Profile of Elraglusib Most adverse events when used as monotherapy were reported as mild to moderate • Transient visual impairment described as transient alterations in color and skin tones under fluorescent light • No permanent changes to eye structure or vision • Visual impairment and fatigue are the two most frequent adverse events attributed to elraglusib • Visual impairment decreases after a few cycles of treatment Key Takeaways

9 Phase 2 – Actuate 1801 Part 3A • Simon’s two - stage design - Stage 1 • 1 st line metastatic pancreatic cancer ( mPDAC ) • Evaluate combination of elraglusib and gemcitabine/nab - paclitaxel ( GnP ) • First 23 consecutively evaluable patients defined as analysis set n= 29 after replacing non - evaluable patients (EE population) • 2 CRs confirmed • 9 PRs confirmed • DCR: 52%, ORR: 38% • Met Simon’s stage 1 threshold of DCR > 50% • 42 total patients enrolled (ITT) Evaluation of best overall response and CA19 - 9 in ITT • Evidence for clinical activity based on tumor and CA19 - 9 response Based on these data, we pivoted to a Phase 2 RCT • N=286 • Randomized (2:1), controlled • Elraglusib + GnP vs GnP alone 1st Line Treatment of mPDAC RCT: randomized , controlled trial; PDAC: pancreatic ductal adenocarcinoma ; ITT: intent to treat ; mITT : modified intent - to - treat ; EE: efficacy evaluable ; CR: complete response ; PR: partial response ; DCR: disease control rate; ORR: overall response rate;

10 Phase 2 RCT • Primary endpoint: OS • Secondary endpoints: ORR, DOR, PFS • Total enrollment: 286 (completed Jan 2024) • Sample size based on increase in 1 year OS from 35% in GnP to 55% in elraglusib / GnP with α =0.05; 232 patients needed for 80% power Predefined Safety Population Draft unaudited data as of April 30, 2024 Phase 2 RCT in First - Line Metastatic PDAC Analysis of the interim data from Actuate - 1801 3B is based on the study statistical analysis plan for informal interim data analysis when >50% of the patients in the GnP control group progressed and were no longer receiving GnP . The final data and results may change as the study continues through completion GnP (78) Elraglusib/ GnP (155) OS mOS (months) 7.3 12.2 HR=0.60; log - rank p=0.012 Events (% events) 42 (53.8%) 53 (34.2%) 12 - month OS (%) 15.5 52.5 18 - month OS (%) 0 20.5 24 - month OS (%) 0 13.6 PFS mPFS (months) 4.6 4.8 HR=0.90; P=NS Events (% events) 50 (64.1%) 79 (51%) ORR n (%) 12 (24%) 32 (30.8%) Evaluable for response RCT: randomized, controlled trial; PDAC: pancreatic ductal adenocarcinoma; OS: overall survival; ORR: overall response rate; DOR: duration of response; PFS: progression - free survival

11 Phase 2 RCT in First - Line Metastatic PDAC Best Overall Response Waterfall Plots Predefined Safety Population Draft unaudited data as of April 30, 2024 The final data and results may change as the study continues through completion

12 • Actuate 1801 Part 1 evaluated elraglusib as a single agent • Extraordinary results for two melanoma patients in the study • First objective response reported in patient treated with 5 mg/kg elraglusib monotherapy • Metastatic melanoma diagnosed in 2018; widely metastasized to the brain, lungs, bones, muscles, stomach, lymph nodes, pancreas and adrenal glands. • Refractory to all FDA - approved standard therapies, including several checkpoint inhibitors and BRAF / MEK inhibitor • After 12 Weeks on elraglusib : Brain MRI showed complete response (CR) by RANO criteria, PET scan showed complete metabolic response (“CMR”). • Durable CMR ongoing (>5.0 years as of February 1, 2024 ) • Refractory, metastatic melanoma identified as clinical indication for elraglusib development • A second patient receiving single agent elraglusib has ongoing stable disease (SD) (3.1 years as of last documented alive date) • Also f ailed all FDA - approved standard therapies including immune checkpoint inhibitors and several experimental treatments • Patients receiving chemotherapy salvage after anti - PD - 1 treatment have a mOS of 6.9 months across all chemotherapy tested 1 • Potential for biomarker enrichment to improve probability of success Combination Key Histologies mOS (1801) Elraglusib /Gemcitabine/ nab - paclitaxel Metastatic Pancreatic Cancer ( mPDAC ) 15.3 months (Part 3A) 12.2 months (Part 3B) Elraglusib Monotherapy Refractory, Metastatic Melanoma 9.1 months Elraglusib /Irinotecan Refractory, metastatic Colorectal 6.9 months 12 weeks on elraglusib leads to Complete Response by PET - MRI. Cystic lesions observed in place of prior tumor Clinical Activity in Areas of High Unmet Need in 1801 Part 1 and 2 1. Goldinger at el., Eur J Cancer 2022; 162: 22.

13 • Seven patients were enrolled in Actuate - 1902 and appear to have metastatic, refractory Ewing and Ewing - like sarcoma and had disease progression on their last treatment regimen prior to joining the study • All seven patients received the combination of elraglusib+cyclophosphamide /topotecan in 1902 • Four out of seven patients had received two or more previous chemotherapy regimens • One patient had CR at their 1st scan as Best Overall Response (BOR) • Stopped all treatments after four months and continues to be in complete remission with no evidence of disease almost two years after termination of treatment • One patient had BOR of CMR (Complete Metabolic Response, no detectable lesions by FDG - PET); • One patient had BOR of PR (52% reduction in tumor) • Two patients had BOR of SD and one patient had BOR of PD • Four patients remain alive and three continue on treatment There are currently no treatment regimens that meaningfully extend life in Ewing sarcoma patients with metastatic, refractory disease P hase 1/2 study (Actuate - 1902) in pediatric cancer patients with recurrent/refractory solid cancer s Patients that have metastasis and disease recurrence after chemotherapy have short survival of 3 - 8 months 1 Clinical Responses in Areas of High Unmet Need - Pediatric Oncology Objective responses and durable survival highlight development opportunity in Ewing sarcoma 1. Van Mater and Wagner. Onco Targets Ther . 2019;12:2279 - 2288.

14 • Single agent dose escalation (Actuate - 1801 Part 1) was evaluated in 67 patients in 15 different cancer types 1 • 35/67 subjects were enrolled at the three highest doses (9.4, 12.4 and 15 mg/kg) • Patients were advanced, refractory patients that had been heavily pre - treated [median 3 (1 - 13)] • A large number of patients had prolonged overall survival (OS) and some tumor shrinkage even of it did not reach level of an obj ective response at these higher doses of elraglusib single agent • Similar dose - response observed with chemotherapy combinations in Actuate - 1801 Part 2 • mOS 7.7 month in Actuate - 1801 Part 1 benchmarks favorably with published data for clinically active agents in Phase 1 (mOS~8 - 10 mon ths 2,3 ) Best Overall Response by Cancer Histology in Part 1 Higher Doses of Elraglusib Appear Associated with Better Overall Survival 1. Carneiro et al Clin Cancer Res 2023: 30: 522 2. Menon et al., 2022 Cancer Rep (Hoboken); 5: e1465 3. Paluri et al. Scientific Rep 1801 Part 1 Best Overall Response Overall Response by Dose 8 months CR=complete response; PR=partial response; SD - stable disease; all response assessments per RECIST 1.1.

15 • Range of clinical benefit for elraglusib injection is hypothesized at 5 mg/kg and above based on PK data in patients 1 • Exceeds in vitro IC50 for tumor cell line death/apoptosis in pre - clinical studies for >12 hours • These doses lead to plasma exposure of elraglusib of up to 87,850 ng•h /mL Dose mg/kg n Cmax ng/mL Tmax H AUC24 ng•h /mL AUC72 ng•h /mL AUC∞ ng•h /mL λ z 1/h t1 /2 h CL L/h/kg Vz L/kg 1 2 - 3 560.5 1.067 2,961 6,145 4,648 0.1027 16.76 0.2854 4.427 2 5 - 5 1 242 1.110 5 932 9 271 8 002 0.05622 15.63 0.2915 5.529 3.3 4 - 5 1,930 1.577 11,571 15,150 13,097 0.08754 11.33 0.2775 4.262 5 5 - 5 1 896 2.200 15 191 23 771 29 335 0.03094 31.93 0.2067 7.605 7 5 - 7 4,027 1.388 30,151 48,433 47,971 0.04612 24.75 0.1835 5.555 9.3 7 - 8 4 146 1.036 31 160 50 405 63 358 0.03827 28.79 0.1953 6.446 12.37 5 - 5 6 912 2.080 44 094 84 381 86 579 0.04856 15.24 0.1881 4.090 15 1 - 2 4,300 1.067 62,376 84,367 87,580 0.02908 36.18 0.1713 3.717 Plasma Pharmacokinetics (PK) after a Single IV Dose in Actuate - 1801 Part 1 Elraglusib Clinical Pharmacology Supports Additional Dose Exploration 1. Carneiro et al Clin Cancer Res 2023: 30: 522 Mean Plasma 9 - ING - 41 ( elraglusib ) Concentration - Time Profiles in Actuate - 1801 Part 1 0 500 1000 1500 2000 2500 3000 0 2 4 6 8 10 12 14 16 18 20 22 24 Plasma 9 - ING - 41 (ng/mL) Time Since Start of Infusion (hours) 3.3 mg/kg 9 - ING - 41 Cyc 1, Day 1 Cyc 1, Day 8 Cyc 2, Day 1 Cyc 2, Day 8 0 500 1000 1500 2000 2500 3000 0 2 4 6 8 10 12 14 16 18 20 22 24 Plasma 9 - ING - 41 (ng/mL) Time Since Start of Infusion (hours) 5.0 mg/kg 9 - ING - 41 Cyc 1, Day 1 Cyc 1, Day 8 Cyc 2, Day 1 Cyc 2, Day 8 Target Plasma Profile (1 m M) Target Plasma Profile (1 m M) Target Plasma Profile (1 m M)

16 • Several possible oral dosage forms may allow potential expansion into pediatric cancer indications and adult indications where standard of care is oral • May improve compliance and patient experience in indications where long DCR is observed • Decreased cost of manufacturing at commercial scale compared to IV formulations • Phase 1 Study of Oral Solution in Normal Healthy Volunteers (NHV) recently completed • Oral Solution vs IV >50% bioavailability when dosed with food • Exposure and pharmacodynamic effects exhibited in fed/fasted patients • Phase 1 dose escalation study using Elraglusib Oral Tablet in advanced cancer patients (not healthy volunteers) scheduled to begin enrollment in 2H24 Fed State vs IV = 51% BA Fasted State vs IV = 17% BA Elraglusib Oral Formulations Oral elraglusib formulations have been developed that provide similar drug exposures to current IV

17 Elraglusib Oral Tablet Plasma Exposure (AUC) at MTD is similar to the Highest Dose of elraglusib Injection tested to date Route Potency Dose Number Target Dose (mg/kg) Actual Dose (mg/kg) Half - life ( hr ) T max ( hr ) C max (ng/mL) AUC last ( hr *ng/mL) Dose - limiting Toxicity IV N/A 1 10 10 2.63 0.0830 6,560 22,300 No Oral 250 mg 2 25 24.5 3.01 4.50 6,090 77,000 No ( MTD ) Oral 500 mg 3 50 49.9 7.63 6.00 9,230 137,000 Yes • Pharmacokinetics to date have been largely dose - proportional • Elraglusib Oral Tablet will be given daily, which should achieve steady state plasma levels of drug • Elraglusib Oral Tablet should achieve daily exposures that are similar to what was previously delivered twice weekly using th e I V formulation • Flat oral dosing vs IV dosing based on weight simplify use and may improve patient compliance • MTD in dogs after a single dose is approximately 25 mg/kg elraglusib Oral Tablet 250 mg • Population PK studies have demonstrated that elraglusib does not increase plasma levels of any of the chemotherapy backbones evaluated to date (gemcitabine, nab - paclitaxel, irinotecan, cyclophosphamide/topotecan) • These studies have also demonstrated that the only known toxicity observed to date with elraglusib Injection have correlated wit h plasma exposure is the visual impairment • Elraglusib Injection did not accumulate in plasma when given on Days 1 and 4 in Actuate - 1801 Part 1 and 2 • This will allow further exploration of risk - benefit, dose and anti - cancer activity in indications identified as promising in Act uate - 1801 Elraglusib Oral Tablet Exceeds Plasma Exposures of Elraglusib Injection

18 IV Program Phase 2 PDAC RCT Completion of enrollment. Part 3A paper ODD & Fast Track Ewing (EWS) EMA PRIME FDA Type D PFS in >80% / OS in 70% of control patients PDAC Topline data EWS PFS in 70% of control patients. 1902 Phase 2 amendment completed to focus on Ewing Request Type B Meeting to discuss EWS AA/ BTD EMA advice meeting PDAC ODD PDAC EMA/COMP ODD EWS EMA/COMP Initiate planning of confirmatory Phase 3 trial Topline data PDAC January April / May June July June December October November 2024 January 2025 Key Near Term Anticipated Development Plans and Milestones

19 Key Near Term Anticipated Development Plans and Milestones Oral Program GMP manufacturing of 250 mg Tablets Initiation of Phase 1 dose escalation trial, adult (AUS) Phase 2 Refractory MM Phase 2 study GMP Release of Tablets PK results from Phase 1 Phase 2 Refractory CRC / NSCLC Phase 2 studies (funding dependent) January March October / November July / August 2024 Q1 2025 Note: The initiation and completion of the Oral Program studies are subject to receipt of adequate funding
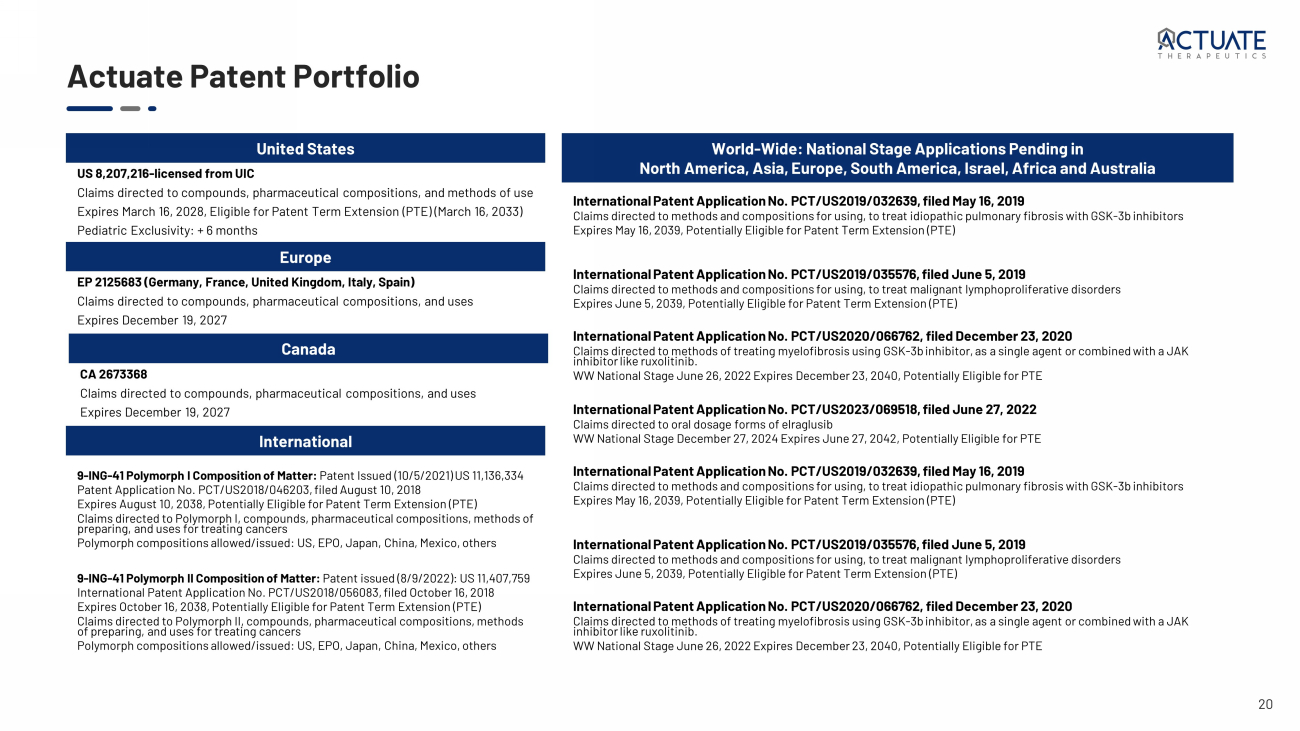
20 9 - ING - 41 Polymorph I Composition of Matter: Patent Issued (10/5/2021) US 11,136,334 Patent Application No. PCT/US2018/046203, filed August 10, 2018 Expires August 10, 2038, Potentially Eligible for Patent Term Extension (PTE) Claims directed to Polymorph I, compounds, pharmaceutical compositions, methods of preparing, and uses for treating cancers Polymorph compositions allowed/issued: US, EPO, Japan, China, Mexico, others 9 - ING - 41 Polymorph II Composition of Matter: Patent issued (8/9/2022): US 11,407,759 International Patent Application No. PCT/US2018/056083, filed October 16, 2018 Expires October 16, 2038, Potentially Eligible for Patent Term Extension (PTE) Claims directed to Polymorph II, compounds, pharmaceutical compositions, methods of preparing, and uses for treating cancers Polymorph compositions allowed/issued: US, EPO, Japan, China, Mexico, others US 8,207,216 - licensed from UIC Claims directed to compounds, pharmaceutical compositions, and methods of use Expires March 16, 2028, Eligible for Patent Term Extension (PTE) (March 16, 2033) Pediatric Exclusivity: + 6 months EP 2125683 (Germany, France, United Kingdom, Italy, Spain) Claims directed to compounds, pharmaceutical compositions, and uses Expires December 19, 2027 CA 2673368 Claims directed to compounds, pharmaceutical compositions, and uses Expires December 19, 2027 Actuate Patent Portfolio International Patent Application No. PCT/US2019/032639, filed May 16, 2019 Claims directed to methods and compositions for using, to treat idiopathic pulmonary fibrosis with GSK - 3b inhibitors Expires May 16, 2039, Potentially Eligible for Patent Term Extension (PTE) International Patent Application No. PCT/US2019/035576, filed June 5, 2019 Claims directed to methods and compositions for using, to treat malignant lymphoproliferative disorders Expires June 5, 2039, Potentially Eligible for Patent Term Extension (PTE) International Patent Application No. PCT/US2020/066762, filed December 23, 2020 Claims directed to methods of treating myelofibrosis using GSK - 3b inhibitor, as a single agent or combined with a JAK inhibitor like ruxolitinib . WW National Stage June 26, 2022 Expires December 23, 2040, Potentially Eligible for PTE International Patent Application No. PCT/US2023/069518, filed June 27, 2022 Claims directed to oral dosage forms of elraglusib WW National Stage December 27, 2024 Expires June 27, 2042, Potentially Eligible for PTE International Patent Application No. PCT/US2019/032639, filed May 16, 2019 Claims directed to methods and compositions for using, to treat idiopathic pulmonary fibrosis with GSK - 3b inhibitors Expires May 16, 2039, Potentially Eligible for Patent Term Extension (PTE) International Patent Application No. PCT/US2019/035576, filed June 5, 2019 Claims directed to methods and compositions for using, to treat malignant lymphoproliferative disorders Expires June 5, 2039, Potentially Eligible for Patent Term Extension (PTE) International Patent Application No. PCT/US2020/066762, filed December 23, 2020 Claims directed to methods of treating myelofibrosis using GSK - 3b inhibitor, as a single agent or combined with a JAK inhibitor like ruxolitinib . WW National Stage June 26, 2022 Expires December 23, 2040, Potentially Eligible for PTE World - Wide: National Stage Applications Pending in North America, Asia, Europe, South America, Israel, Africa and Australia United States Europe Canada International

21 Capitalization As of March 31, 2024 Pre - IPO Cap Table (as converted, assumes $9.00 offering price and 1:1.8 reverse split) Common Stock 16,211,835 (1) Warrants (WAEP: $10.32) 94,599 Options (WAEP: $2.97) 393,346 Fully Diluted Shares Outstanding 16,699,780 1) Includes the conversion of all outstanding shares of convertible Series A, B, and C preferred stock; net exercise of in - the - mone y Series B Warrants; the conversion of Bridge Notes (principal amount $5.5 million) upon the IPO; and a 1:1.8 reverse stock split of our common stock immediately prior to the of fer ing.

22 Andrew Mazar, PhD – Chief Operating Officer and Scientific Co - Founder • Co - founder, Chief Scientific Officer and Director, Monopar Therapeutics, Inc. (Nasdaq: MNPR) • Entrepreneur - in - Residence; Professor of Pharmacology; Founding Director, Center for Developmental Therapeutics, Northwestern Uni versity • Chief Scientific Officer, Attenuon , LLC • Internationally recognized expert in cancer metastasis and translational oncology • Eleven drugs from discovery through Phase 2 • >250 peer - reviewed publications and book chapters and inventor on > 70 patents • Serial entrepreneur with seven start - ups founded Daniel M. Schmitt – Chief Executive Officer and Founder • 3 0 + years of biotechnology and pharmaceutical experience across senior executive roles • Led and contributed to the successful development and launch of multiple pharmaceutical products • Exosurf, Zovirax, Valtrex, Adenoscan, Ambisome, Duraclon, Campath, Abraxane, enTrust • Executed ~1B+ in milestone value through licensing, acquisition, and development deals Paul Lytle – Chief Financial Officer • 30+ years of finance and accounting experience • 25+ years of public company experience for Nasdaq listed companies • Served as co - founder, CFO, and director for multiple biotech companies • Raised in excess of $500 million in net proceeds from various equity and debt offerings Steven D. Reich , MD – Sr VP, Clinical Development and Acting Chief Medical Officer • Oncology drug development executive leader for commercial clinical development and strategy • Directed multi - national medical research groups within pharmaceutical/biotechnology companies and CRO • Lead investigator for Phase I - III trials and designed and managed Phase I - IV trials for industrial sponsors • Headed the clinical research programs leading to multiple US, Canadian, and European drug approvals • Epogen, Targretin, Panretin , Fludara , Inlyta Seasoned and Successful Leadership Experienced leadership team with demonstrated ability to develop and commercialize cancer drugs
23 Leading Therapeutic Profile Extensive data on activity from leading research institutions and promising clinical data in multiple cancer histologies Investment Highlights Significant Unmet Needs Developing elraglusib to address therapeutic shortcomings in key difficult - to - treat and refractory tumors Complementary Mechanisms of Action Focus on mediating cancer cell survival and chemoresistance through regulation of NF - kB and regulating antitumor immune response Robust IP Portfolio Expansive, global patent portfolio with significant exclusivity runway Clearly Defined Regulatory Path Multiple key regulatory designations available (Fast Track, Orphan Drug, Rare Pediatric) with registration path clinical trials underway and in development Seasoned Leadership Team Distinguished leadership and recognized world leading scientific advisory team

24