UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
___________________________
FORM 10-K
___________________________
(Mark One)
| | | | | |
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2023
OR
| | | | | |
| ☐ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission File Number: 001-40606
___________________________
SERA PROGNOSTICS, INC.
(Exact Name of Registrant as Specified in its Charter)
___________________________
| | | | | | | | |
| Delaware | | 26-1911522 |
(State or other jurisdiction of
incorporation or organization) | | (I.R.S. Employer
Identification No.) |
2749 East Parleys Way, Suite 200 Salt Lake City, Utah | | 84109 |
| (Address of principal executive offices) | | (Zip Code) |
Registrant’s telephone number, including area code: (801) 990-0520
___________________________
Securities registered pursuant to Section 12(b) of the Act:
| | | | | | | | | | | | | | |
| Title of each class | | Trading Symbol(s) | | Name of each exchange on which registered |
| Class A Common Stock, $0.0001 par value per share | | SERA | | The Nasdaq Stock Market LLC |
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No o
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes x No o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| | | | | | | | | | | |
| Large accelerated filer | o | Accelerated filer | o |
| Non-accelerated filer | x | Smaller reporting company | x |
| | Emerging growth company | x |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. o
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. o
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. o
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b). o
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No x
The aggregate market value of the registrant’s Class A common stock held by non-affiliates of the registrant, computed by reference to the closing price as reported on the Nasdaq Stock Exchange on June 30, 2023, the last business day of the registrant’s most recently completed second fiscal quarter, was approximately $91.7 million. As of March 15, 2024, the registrant had 31,457,902 and 967,759 shares of Class A and B common stock, $0.0001 par value per share, outstanding, respectively.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive proxy statement relating to its 2024 annual meeting of stockholders (the “Proxy Statement”) are incorporated by reference into Part III of this Annual Report on Form 10-K where indicated. The Proxy Statement will be filed with the Securities and Exchange Commission within 120 days after the end of the registrant’s fiscal year ended December 31, 2023.
TABLE OF CONTENTS
“Sera,” “PreTRM,” “The Pregnancy Company” and our logo are our trademarks. All other service marks, trademarks, and trade names appearing in this Annual Report on Form 10-K are the property of their respective owners. We do not intend our use or display of other companies’ trade names, trademarks, or service marks to imply a relationship with, or endorsement or sponsorship of us by, these other companies. Solely for convenience, trademarks and tradenames referred to in this Annual Report on Form 10-K may appear without the ® or ™ symbols, but such references are not intended to indicate in any way that we will not assert, to the fullest extent under applicable law, our rights, or that the applicable owner will not assert its rights, to these trademarks and tradenames. Unless the context otherwise requires, we use the terms “Sera,” “Company,” “we,” “us” and “our” in this report to refer to Sera Prognostics, Inc.
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This discussion contains certain forward-looking statements within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended, or the Exchange Act. In some cases, you can identify forward-looking statements by words such as “anticipate,” “believe,” “contemplate,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “predict,” “project,” “seek,” “should,” “target,” “will,” “would,” or the negative of these words or other comparable terminology. These forward-looking statements include, but are not limited to, statements about:
•estimates of our addressable market, market growth, future revenue, key performance indicators, expenses, capital requirements, and our needs for additional financing;
•our expectations regarding the rate and degree of market acceptance of our PreTRM test;
•the impact of our PreTRM test on the field of bioinformatics and proteomics and the size and growth of the addressable bioinformatics and proteomics market;
•our ability to obtain funding for our operations;
•our ability to manage and grow our business and commercialize our PreTRM test;
•our ability to develop and commercialize new products;
•our ability to retain the continued service of our key professionals and to identify, hire, and retain additional qualified professionals;
•the pricing and reimbursement of our products;
•the implementation of our business model, strategic plans for our business, products and technology;
•the scope of protection we are able to establish and maintain for intellectual property rights covering our product candidates and technology;
•developments relating to our competitors and our industry;
•the accuracy of our estimates regarding expenses, capital requirements, and needs for additional financing;
•conditions in general economic and financial markets; and
•our financial performance.
These forward-looking statements are subject to a number of risks, uncertainties, and assumptions, including those described in the “Risk Factors” section and elsewhere in this report. Moreover, we operate in a very competitive and rapidly changing environment, and new risks emerge from time to time. It is not possible for our management to predict all risks, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statements we may make. In light of these risks, uncertainties, and assumptions, the forward-looking events and circumstances discussed in this report may not occur and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements.
You should not rely upon forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable as of the date of this report, we cannot guarantee that the future results, levels of activity, performance or events and circumstances reflected in the forward-looking statements will be achieved or occur. We undertake no obligation to update publicly any forward-looking statements for any reason after the date of this report to conform these statements to new information, actual results or to changes in our expectations, except as required by law.
PART I
Item 1. Business
Overview
We are a women’s health company utilizing our proprietary proteomics and bioinformatics platform, and significant data resources to improve maternal and neonatal health by discovering, developing, and commercializing blood-based biomarker tests, and predictive analytic products and services. Our vision is to deliver pivotal and actionable information to pregnant women, their physicians, and health care payers to significantly enhance a mother’s pregnancy journey, improve maternal and neonatal health, and dramatically reduce health care costs. We believe that our method of combining the disciplines of proteomics and bioinformatics with rigorous clinical testing, data, and economic analysis enables us to provide physicians, patients, and consumers with personally insightful, clinically meaningful, and economically impactful information designed to improve the pregnancy experience and outcomes for mothers and babies.
There are approximately 140 million births globally each year, and approximately 3.7 million births annually in the United States. Of these, it is estimated that as many as 30% are affected by various complications (i.e., a high-risk pregnancy), including: preterm birth, preeclampsia, fetal growth restriction, stillbirth, hypertension of pregnancy, gestational diabetes, and others. In many cases these complications have profound short- and long-term health consequences for the mother and baby. These health consequences of preterm birth alone are estimated to be approximately $25 billion annually in the United States. This underscores that existing methods to predict adverse pregnancy outcomes are insufficient for timely and effective proactive management for the vast majority of high-risk pregnancies. We believe that positive patient outcomes are the result of appropriate care, and the primary differentiator of patient care should be based on a determination of risk informed by a number of factors including our novel diagnostic tests.
Our first commercial product, the PreTRM test, is the only broadly validated, commercially available blood-based biomarker test to accurately predict the risk of a premature delivery, also known as preterm birth. The PreTRM test is a non-invasive blood test given to a pregnant woman, carrying a single fetus, during weeks 18 through 20 of gestation that provides an accurate prediction of the expectant mother’s risk of delivering spontaneously before 37 weeks’ gestation. Our commercialization strategy includes streamlining patient access to the test by improving specimen acquisition and transport and conducting clinical trials to demonstrate the health and economic benefits of early and accurate detection of preterm birth risk coupled with well-recognized interventions in higher risk patients. Our key clinical trials to date include the Prediction and Prevention of Preterm Birth, or the PREVENT-PTB Study, Serum Assessment of Preterm Birth Outcomes Compared to Historical Controls study, or the AVERT PRETERM TRIAL, and the Prematurity Risk Assessment Combined With Clinical Interventions for Improving Neonatal outcoMEs study, or the PRIME study. Manuscript results of these studies demonstrate consistency in the reported beneficial impact of the PreTRM test and treat strategy. Specifically, this includes evidence of a prolongation of gestation, shortened hospital or NICU length of stay, and improvements in measures of neonatal morbidity/mortality. A model that is emerging is that by identifying and intervening on at-risk pregnancies, not identifiable by other approaches, babies destined for premature delivery remain in utero longer. This prolongation of gestation in the preterm period leads to more mature babies that require shorter hospital/NICU stays due to improved neonatal health. The PRIME study, for which enrollment was stopped due to efficacy at the interim analysis and is being prepared for publication, includes the same primary and secondary endpoints as the AVERT PRETERM TRIAL and affords the continued assessment of this model.
We have built an advanced, proprietary, and scalable proteomics and bioinformatics platform to characterize the biology of pregnancy and to discover and validate key protein biomarkers found in blood that are highly accurate predictors of dynamic changes that occur during pregnancy. By incorporating our proprietary technology platform into our rigorous data-driven development process, we have created a differentiated approach for effectively addressing major milestones, conditions, and features of pregnancy. We believe our large and growing pregnancy dataset (clinical, demographic, and proteomic) is a substantial asset for understanding pregnancy complications, health inequities, and the personal pregnancy journey. We envision that our comprehensive approach will enable us to fully characterize one of the most important periods in the lives of women and their babies, and will help to improve each of their well-being.
We are actively discovering and developing several additional biomarker tests to predict other specific major conditions of pregnancy, such as a pregnancy risk prediction panel test. We believe these tests have the potential to offer significant health benefits to women and their babies. Among other products, we are developing a test designed to provide a more accurate estimate of the delivery date for expectant mothers for the purposes of planning maternity leave, required support, travel arrangements, and related considerations.
Our Proprietary Technology Platform
The complexities of the biological processes occurring during pregnancy have been a major obstacle in developing effective tests for pregnancy-related conditions. We are working to overcome this obstacle through our development of a proprietary technology platform consisting of biobanks, advanced mass spectrometry, immunoassays, and other proteomic analytic methods and bioinformatics, which enables superior characterization of the biology of pregnancy and more accurate prediction of pregnancy outcomes.
An analysis of protein pathways and expression at various points during pregnancy reveals the constantly evolving and dynamic changes affecting both the mother and the baby. Earlier detection of changes in protein expression indicating the emergence of adverse pregnancy outcomes can enable proactive management of those conditions. A fundamental component of our platform is our proprietary biobank, consisting of comprehensive, clinically and demographically annotated specimens collected from thousands of pregnant U.S. women, representing the broad demographic and geographic diversity inherent in the U.S. population. This differentiated resource enables us to develop and broadly validate our predictors. Further biobank diversity is also provided through our scientific collaborations with leading maternal fetal medicine experts around the globe, enabling us to analyze specimens collected from patients in the United States, Europe, Asia and Africa. In strict adherence to the authoritative National Academy of Medicine, or NAM, guidelines, we apply our innovative mass-spectrometry and other proteomic analytical methods and our protein information network knowledge to probe biobank specimens for meaningful protein expression changes. We then subject the data to detailed bioinformatics analysis and use advanced tools, such as machine learning and artificial intelligence, to find relationships between various proteins and to discover important predictors.
Our Discovery, Development, and Commercialization Approach
Our product discovery and development approach is based on rigorous science and health-based economic analyses as we discover, develop and commercialize biomarker tests and predictive analytic products and services designed to transform pregnancy-related care for patients, doctors and payers. We have initially applied our platform and capabilities to address the problem of preterm birth, given its profound health and economic impacts worldwide. In the future, we may use this technology to develop products for a number of health conditions other than premature birth. Our development and commercialization strategy also involves transitioning some products from proteomic discovery platforms (such as mass spectrometry) to immunoassays, which we believe also have low costs, high-throughput, and ease of implementation. Technology development also includes removing bottlenecks in specimen collection and shipment by use of whole-blood collection and ambient shipping.
We use the following multifaceted approach in our research, development and commercialization efforts:
•Significant Unmet Need: We select specific conditions or features of pregnancy that are clinically and personally meaningful and economically important and with significant unmet needs that lack effective solutions.
•Proteomic and Bioinformatics Platform: We utilize our platform to understand the biology underlying selected pregnancy-related conditions in order to discover, verify and broadly validate high-performing predictive biomarker tests and predictive analytic products and services.
•Immunoassays: We identify antibodies to discovered pregnancy biomarkers and develop immunoassays for use in our CLIA laboratory and eventual use in ex-US territories.
•Whole-Blood Collection and Ambient Shipment: We migrate from discoveries made in our serum pregnancy biobank and temperature-controlled specimen shipment to whole-blood collection and ambient shipment.
•Demonstration of Health and Economic Impact of Our Test and Treat Strategy: We believe a critical element of our success will be to demonstrate the beneficial health and economic impacts of using the information provided by our biomarker tests.
•Societal Guidelines: We believe that broad market adoption of a product benefits from the product being included in clinical societal guidelines and therefore we work closely with organizations such as the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists, as we keep them apprised of our accumulating evidence development.
•Payment and Reimbursement: We have focused on building third-party reimbursement for early commercialization of our clinical tests, by seeking to leverage the health and economic benefits conferred by our biomarker approach to gain reimbursement from integrated systems, large physician practices, and major health insurance payers. Other products or market segments may be more conducive to direct patient or consumer payment models.
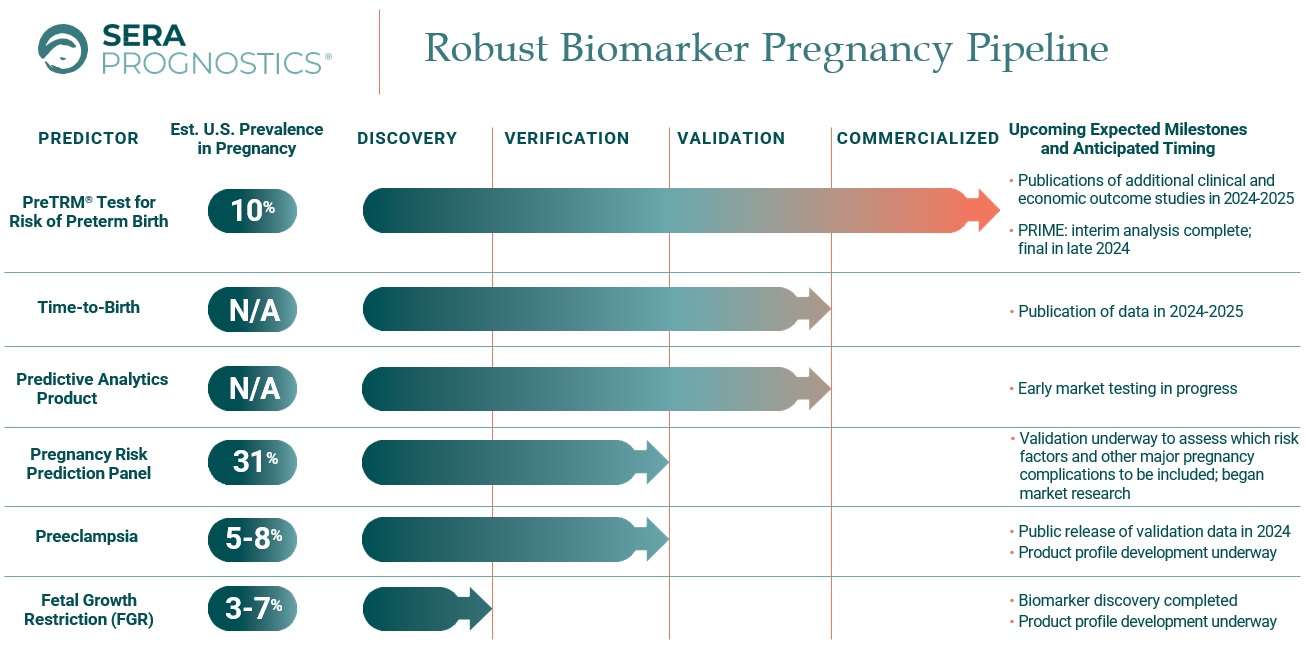
Our Pipeline
We are developing a robust pipeline of novel blood-based biomarker tests for a number of major pregnancy related conditions beyond preterm birth by leveraging the biological insights provided by our proprietary technology platform. Our product candidates are designed to accurately predict and enable better management of a range of serious pregnancy-related conditions. We believe these product candidates, if successfully developed, have the potential to address significant unmet needs by providing more accurate detection of these pregnancy-related conditions and providing patients with meaningful information and physicians with earlier opportunities for interventional treatment.
Our biomarker pregnancy pipeline consists of the following:
Our Strengths
We attribute our success and future growth prospects to the following:
•Our differentiated approach to understanding and addressing major conditions of pregnancy. We take a focused and data-driven approach based on rigorous science to understand the biology of pregnancy and the health and economic impacts of major pregnancy conditions. Our approach involves conducting controlled trials and health economic analyses to demonstrate the beneficial health and economic impacts of using the information provided by our products. We also work with leading health economists and organizations to build rigorous models that describe how the application of our products impacts both health and economic outcomes. Leveraging the demonstrated short- and long-term health and economic benefits of our approach, we aim to gain reimbursement from integrated systems, large physician practices, self-insured employers and major health insurance payers by working with them to demonstrate the benefits of using our products. We also expect to explore alternative payment models for some products and market segments. We will then seek to capitalize on reimbursement decisions to facilitate obtaining widespread commercial coverage of our biomarker tests from other health care payers, while also expanding any successful alternative payment models for these and other products.
•Our proprietary and scalable proteomics, bioinformatics platform technology, and clinical outcome data creates clinically meaningful and economically impactful predictions for pregnancy. We believe our proprietary proteomic and bioinformatics technology platform has the potential to enable critical advances in the management of pregnancy and its outcomes. Our platform consists of biobanks, advanced mass spectrometry, immunoassays, and other proteomic analytic methods and bioinformatics, which enables superior characterization of the biology of pregnancy and accurate characterization of pregnancy outcomes and features. Intrinsic to our technology expertise is the ability to identify antibodies to proteomically-discovered biomarkers to allow transition from mass spectrometry to simple, high-throughput, lower-cost immunoassay approaches over time. We believe this platform has the potential to address significant unmet needs in the large, underserved market for the prediction of outcomes associated with pregnancy. Our research allows for the development of testing technology on other platforms in cases when partnering with leading instrument providers proves to be the most effective route to broad-based adoption for any of our products.
•Whole-Blood Collection and Ambient Shipment. We have years of experience evaluating whole-blood collection approaches and methods of ambient shipment. We leverage our discovered serum biobank-based clinically meaningful predictions to translate to whole-blood collection and ambient specimen shipment. This can lower costs, ease patient/consumer experience and accelerate market penetration.
•The PreTRM Test, which is the only broadly validated, commercially available blood test proven to predict the risk of an individual woman to deliver prematurely. The predictive performance of the PreTRM biomarkers has been extensively validated in diverse populations and geographies and enables earlier proactive care addressing higher preterm birth risk that occurs among the 3.7 million annual singleton pregnancies in the United States. We believe that based on our growing body of evidence regarding the clinical and economic benefits of the PreTRM test, as greater payer and physician adoption and supportive medical society guidelines occur, the PreTRM test has the potential to become an important standard of care for preterm birth.
•Collaboration with Elevance Health. We have contracted for early payment for the PreTRM test through our commercial collaboration with Elevance Health. We believe this and other collaborations may help with broader market adoption through coverage decisions by major payers.
•Broad pipeline covering additional significant conditions of pregnancy. We are also developing a novel pipeline of blood-based biomarker tests and predictive analytic products and services directed at a number of major pregnancy-related conditions and features beyond preterm birth by leveraging the biological insights provided by our proprietary technology platform. We believe these product candidates, if successfully developed, have the potential to address significant unmet needs by providing more accurate detection of these pregnancy-related conditions and features, which in turn can give consumers helpful information about their pregnancy journey and give patients and physicians earlier opportunities for interventional treatment.
•Deeply experienced team in development and commercialization of molecular diagnostics tests and predictive analytic products and services. Our team has decades of experience in building and commercializing molecular diagnostics tests and predictive analytic products and services. We have worked to build a first-class scientific organization capable of harnessing and translating our platform technologies into innovative solutions. We strive to deliver actionable information to pregnant women, their physicians and payers to improve the pregnancy experience and the health of patients as well as the economics of health care delivery. Our experienced discovery and development team performs rigorous bioinformatics analyses and strictly adheres to the authoritative NAM guidelines on how to reliably develop and validate omics predictions made on complex biological data sets. Adhering to these guidelines, in the case of predicting preterm birth, we have been able to document generalizable biomarker predictive performance across independent cohorts of patients from the United States, Europe, Asia and Africa. Reflective of the scientific rigor of our efforts, our scientists have published best practice recommendations for the analysis of preterm delivery data. We believe this will improve the quality of statistical analysis of research data related to proteomic test development, enabling the broad community of statisticians, researchers, clinicians and regulators to better validate predictions prior to their clinical use.
Our Strategy
Our vision is to deliver pivotal and actionable information to pregnant women, their physicians and health care payers to significantly improve the pregnancy experience and maternal and neonatal health, and to dramatically reduce health care costs. Our goal as The Pregnancy Company is to discover, develop and commercialize commercially and clinically
meaningful and economically impactful biomarker tests and predictive analytic products and services designed to improve the pregnancy experience and pregnancy outcomes. We assess product opportunities across physician-ordered, direct-to-consumer and business-to-business commercialization models and both payer-reimbursed, and consumer-pay approaches. We believe it is critical to develop products that will be viewed as cost-effective by payers in order to receive reimbursement for our tests. We aim to accomplish our vision by implementing the following strategies:
•Expand payments for the PreTRM test to a variety of market segments and payment models to maximize the commercial opportunity. We believe that growing payment for the PreTRM test by integrated systems, large physician practices, self-insured employers, major health insurance payers and even patient self-payment models should help drive physicians to more broadly offer the testing to their patients, thereby expanding the number of U.S. pregnancies benefiting from our technology. We also believe that based on our growing body of evidence regarding the clinical and economic benefits of the PreTRM test, our commercial collaboration with Elevance Health, and the anticipated greater payer and physician adoption throughout the United States, the PreTRM test has the potential to create a new standard of care in pregnancies.
•Apply our platform capabilities to broaden our pipeline and develop novel and high-performing products for pregnancy-related conditions and potentially other health conditions. Our proprietary technology platform is designed to provide deep characterization of the biology of pregnancy, which we are using to develop additional products addressing pregnancy outcomes, such as time-to-birth, preeclampsia, gestational diabetes, and other conditions. We plan to leverage the strength of our technology platform and expertise to discover and develop novel and high-performing products that will provide women and physicians more timely and actionable information on pivotal pregnancy conditions and features, which can lead to an improved pregnancy experience and improved maternal and newborn health. In the future, we aspire to expand our product offerings by deeply characterizing the biology of the pregnancy journey.
•Continually enhance the value and capabilities of our proprietary technology platform through ongoing expansion and integration of our biobank and our proteomics and bioinformatics databases. We believe that the breadth and depth of our databases, our unique proteomic analytical techniques, immunoassay capabilities, and our bioinformatics approaches all position us to be the leader in providing important pregnancy information to women and doctors. The continued expansion of our proprietary biobank, together with our innovative proteomic analytical methods and bioinformatics analyses, is designed to enable us to discover and broadly validate new biomarker and predictive analytic products and services for various conditions and features of pregnancy.
•Evolution of our testing, specimen collection and shipping technologies. Market penetration and optimal patient/consumer experience can also be realized by implementation of whole-blood collection technologies and development of ambient specimen shipment approaches. Whole-blood collection can remove laborious specimen processing steps such as centrifugation and enable at-home consumer channels. Ambient specimen shipping removes requirements for temperature-control, which lowers costs, and its simplicity can improve clinical implementation and further streamline at-home collection. For certain products, affinity-capture and/or immunoassay development can minimize overall costs of goods and maximize sample throughput and turnaround time. Intrinsic to our strategy is evolving from discoveries made using mass-spectrometry analysis of our proprietary biobank to identification of antibodies for use in immunoassays.
•Continue building an evidence portfolio of clinical and economic outcomes driven by our products. In addition to completing publications of AVERT and interim PRIME results, we seek to complete economic analyses for both studies and to publish additional outcomes related to the full set of enrolled patients in the PRIME study. Additionally, we plan to demonstrate the results of our test and treat strategy in real-world evidence studies.
•Engage with professional societies. We have historically engaged and will continue working closely with professional societies and guideline setting bodies to advocate for the continued evolution of treatment guidelines to include the latest research and innovations for maternal and newborn health.
•Partner with employers to expand the payer mix for our products. We are partnering with employer cooperative organizations to include our products in benefit packages for maternal care for some of the largest employers in the United States.
•Complement our products with a care coordination offering. We now offer our large institutional customers the care coordination protocol delivered by our dedicated obstetric nurses for all their patients that test at higher risk for preterm birth.
•Build a women’s health commercial infrastructure. We are continually building out commercial, sales, and marketing capabilities to fit the current stage and future life cycle of our product portfolio, including institutional sales, self-insured employer markets, sales operations, and professional as well as consumer directed marketing. When commercial opportunities and market conditions warrant, we will expand our commercial operations to penetrate each market in a cost-effective manner.
•Evaluate strategic partnerships to maximize the value of our product offerings. We may strategically enter into collaborations or other partnerships to maximize the commercial potential of the PreTRM test and the rest of our product portfolio within or outside of the United States. We may explore strategic alliances or collaboration to accelerate the discovery, development, validation and commercialization of our portfolio.
•Build long-term relationships with our expectant mother customers to support their pregnancy journeys. With the expansion of our product portfolio, we have many opportunities to support mothers in their pregnancies. Building an ongoing relationship with our customers via digital channels should allow us to offer more products and solutions, enhance the predictive power of our technology, and increase the return on investment on our customer acquisition cost.
The Biology of Pregnancy
Pregnancy is a highly complex, dynamic process that leads to the formation of a human being. From its beginning, genes, proteins and metabolites are expressed in a coordinated fashion to enable the placenta, the uterus and the mother to support the development of a child during pregnancy. The duration of a term pregnancy is usually between 37 and 42 weeks.
At the inception of pregnancy, the placenta begins its development as a critical organ necessary for a healthy pregnancy for both the baby and the mother. The placenta initially forms and evolves during pregnancy to become a large, highly active metabolic organ conducting numerous vital biological functions through the time of delivery. The placenta is the primary means of communication between the mother and the baby. Life-enabling exchanges of oxygen, nutrients and protective antibodies as well as elimination of wastes are effected by the placenta.
Proteins and protein expression are critical molecular elements in driving and carrying out key processes that take place during pregnancy in both the mother and the baby. Protein expression can, in some cases, become disordered, leading to adverse pregnancy outcomes, such as preterm birth, preeclampsia, gestational diabetes, stillbirth and other conditions. There are approximately 140 million births globally each year. It is estimated that as many as 30% of pregnancies may have complications affecting the mother and/or the baby.
Maternal blood is a window through which maternal, fetal and placental communication can be deciphered. Subtle abnormalities in protein expression in the mother’s blood may provide insights into complications earlier in pregnancy that can be utilized to benefit the mother and the baby. These changes, if appropriately detected and understood, have the potential to predict that the mother and/or baby are trending toward adverse conditions in pregnancy, which can be serious and costly. Timely detection of these subtle changes can enable the application of specific interventions to address the emergence of such complications and thereby improve the health of mothers and babies.
To date, a deeper understanding of the abnormalities of protein expression has been limited by the lack of understanding of the molecular events of the biology of pregnancy. The development of meaningful predictions in pregnancy requires improved methods to better understand such biology.
Building clinically meaningful and economically impactful predictions for pregnancy requires a significant commitment of resources, the proper selection and application of state-of-the-art laboratory technologies, access to well-annotated biologic specimens and advanced bioinformatics capabilities.
Proprietary Technology Platform
We believe our proprietary proteomic and bioinformatics technology platform has the potential to enable critical advances in the management of pregnancy and its outcomes. Our platform consists of biobanks, advanced mass spectrometry and other proteomic analytic methods and bioinformatics, which enables superior characterization of the biology of pregnancy and accurate prediction of pregnancy outcomes. Our platform, built on differentiated tools and capabilities, provides pregnant mothers and their doctors more clinically meaningful and economically impactful predictions of adverse pregnancy outcomes to enable more timely intervention and improve the well-being of both mother and baby.
Proprietary Biobanks
We have built proprietary biobanks of blood specimens and related data over a number of years, which are key resources required to develop a deeper understanding of the biology of normal and adverse pregnancy outcomes. By continuing to aggregate proprietary bioinformatics insights gained from analyses of comprehensively annotated biobank specimens, we are working to develop and commercialize a variety of clinically meaningful and economically impactful biomarker tests for pregnant women and their health care providers.
Our large proprietary U.S. biobank resource was built by collecting blood from thousands of comprehensively annotated blood specimens from patients, which cover a broad range of gestational ages and represent the broad demographic diversity and geographic distribution of pregnant women across the United States. We collected the specimens in two large multi-center trials: our PAPR study, beginning in 2011, and our TREETOP study, beginning in 2016. These two studies prospectively collected specimens, together encompassing weeks 17 through 28 of pregnancy, from women carrying a single baby, and, as “all comers” studies, collected information on a variety of important pregnancy outcomes, including preterm birth, preeclampsia, gestational diabetes and other conditions. These specimens and their associated data are carefully analyzed to discover and develop informative biomarker signatures for intended use pregnancy populations. We continuously work to add new specimens to our biobanks in additional studies, generating greater opportunities for ongoing development of clinically meaningful and economically impactful biomarker predictions.
We believe our work on proprietary biobanks has established us as a leader in proteomic approaches to characterize pregnancy. We also conduct our bioinformatics analyses on additional specimens from other institutions in the United States and abroad. We analyze each specimen by conducting proteomic and other measurements in our laboratory, which generates large sets of biomarker data for each specimen. Through the analysis and evaluation of biomarkers with advanced bioinformatics approaches, we discover novel predictions for various adverse pregnancy outcomes. We then are able to apply these predictions to non-overlapping independent specimens from different biobanks available to us to confirm and validate the accuracy and performance of the predictions. We add to our biobanks on an ongoing basis by continuously analyzing larger numbers of specimens from our own sponsored studies as well as those from collaborations with maternal fetal medicine leaders around the world. We have validated proprietary biomarker signatures consisting of proteins and clinical variables in specimens collected from the United States, Europe, Asia and Africa. We believe that as our database and sets of predictions grow, verifying and validating the predictions can lead to more rapid and efficient development required to commercialize such predictions in the future.
Advanced Mass Spectrometry Approaches
Mass spectrometry is a highly developed analytical technology capable of precise identification, quantification and characterization of proteins. We have developed and applied innovative state-of-the-art mass spectrometry techniques to screen and detect in our bio-specimens the dynamic changes in protein expression occurring in normal and abnormal pregnancy development. Our proprietary proteomics workflows enable detailed and efficient measurements of hundreds of proteins simultaneously from complex matrices, such as blood. We also utilize a variety of other screening techniques to explore and understand the pregnancy proteome, including large- and small-scale immunoassay screens, other ligand-binding assays and RNA analyses, among others. To ultimately validate biomarker performance, we translate and confirm, on our mass spectrometry platform, the findings that we have generated with these other analytical measurement technologies. Our rich and extensive database of omics data, combined with highly annotated clinical information, is analyzed by state-of-the-art bioinformatics capabilities.
Through our innovative approaches and advances in proteomics, we have discovered and validated meaningful predictions for adverse pregnancy outcomes. Importantly, our mass spectrometry process is well-suited not only for discovery and development activities, but also for high volume commercial production through the use of robotics and
automation. Mass spectrometry measurements can be performed on very small blood volumes, which is appealing for patient specimen collection and can lower cost of goods in laboratory analyses. We endeavor to remain at the forefront of the clinical application of mass spectrometry-based proteomics by making advancements in specimen collection/shipping and laboratory processes. We believe that our specific applications of mass spectrometry-based proteomics can be scaled to efficiently and cost-effectively accommodate the growth that we anticipate in addressing the large pregnancy testing market.
We are continually enhancing our analytical techniques. This includes improving customer experience with the identification and validation of whole-blood collection devices, ambient specimen shipping, and laboratory process changes. We continually refine the laboratory process to make it more efficient, lower costs, and improve turnaround time, or TAT. A significant goal in our strategy is the migration to immunoassays in cases where this is advantageous, such as consumer ordered tests or international clinical testing kits. Antibodies are the currency that applies across the immunodiagnostic space as they apply uniformly despite the variations in immunoassay platform technologies. An automated affinity-capture mass-spectrometry, or AC-MS, PreTRM assay is expected to launch in the first half of 2024. This approach uses custom, proprietary antibodies, coupled to magnetic beads to isolate PreTRM analytes for mass spectrometry measurement. AC-MS enables parallel processing of specimens, very short LC-MS analysis times, quicker overall TAT, and lower costs. We continue to evaluate additional antibodies to PreTRM analytes for potential development of sandwich immunoassays (e.g. ELISA) or clinical analyzer-compatible assays. Current efforts also include the identification of antibodies and the development of immunoassays for other pipeline products.
Advanced Bioinformatics
We have assembled a powerful collection of advanced bioinformatics capabilities as a critical component of our platform. Bioinformatics is an essential field of science in which biology, statistics, advanced computational science and information technology are combined to systematically and comprehensively analyze complex biological information. The advanced bioinformatics tools that we apply at great scale to measurements conducted on our biobank specimens to develop high-performing, important predictive algorithms include, but are not limited to: machine learning, artificial intelligence, causal inference, supervised learning methods, dimensionality reduction methods and advanced statistics. As a result of rigorously applying our core expertise and proprietary approaches in bioinformatics, we have discovered high-performing algorithms that reliably distinguish pregnancies with normal protein expression compared to those showing disordered protein expression. Deep bioinformatics insights into the biology of pregnancy have enabled us to discover, verify and validate important predictions of adverse pregnancy outcomes.
We have built an experienced discovery and development team with the deep expertise in science and mathematics necessary to perform rigorous bioinformatics analyses. We strictly adhere to the authoritative guidelines published by NAM on how to reliably develop and validate omics predictions made on complex biological data sets. These guidelines require disciplined validation of predictions to ensure validity and reliability of such predictions before they can be used clinically or commercially. The NAM guidance calls for pre-specifying how the predictions are to be made and then applying testing in completely independent specimen cohorts, in order to be certain that the predictions are valid. Adhering to these guidelines, we have been able to validate that a number of our adverse pregnancy predictors are replicable in independent cohorts of patients residing in United States, Europe, Asia and Africa.
Our Product Discovery, Development and Commercialization Approach
We leverage our proprietary technology platform to develop and commercialize novel, high-performing products that are designed to make a significant difference to pregnant women, doctors and payers. In our product development efforts, we take a focused and data-driven approach based on rigorous science and economics, and in alignment with appropriate regulatory guidelines. Our multi-faceted approach involves the following elements that we apply in the discovery, development and commercialization of our biomarker tests:
•Significant Unmet Need. We select specific conditions of pregnancy that are clinically meaningful and economically important and with significant unmet needs that lack effective solutions. We have initially applied our platform and capabilities to address the problem of preterm birth, given its profound health and economic impacts worldwide. We intend to explore other areas of significant unmet need in pregnancy, including preeclampsia, gestational diabetes and others.
•Proteomic and Bioinformatics Platform. We utilize our platform to understand the biology underlying such conditions in order to discover, verify and broadly validate high-performing predictive biomarker tests. We pursued a multi-year effort to build an extensive biobank resource that we used to discover, verify and validate our first product, the PreTRM test. Thousands of patients were enrolled in two large U.S. multi-center clinical validation studies. Beyond their validation of the PreTRM test, these studies provide a deep view into the care and outcomes of diverse singleton pregnancies across the United States, enabling prediction of various other outcomes. We are continuing to conduct analyses by combining growing biobank data from multiple studies to provide new insights that will be the basis of discovering and developing biomarker predictions for a variety of important conditions of pregnancy.
•Demonstration of Health and Economic Impact of Our Test and Treat Strategy. We believe a critical element of our success will be to demonstrate the beneficial health and economic impacts of using the information provided by our biomarker tests. Our approach involves conducting controlled trials and health economic analyses. In the case of the PreTRM test, an important part of our commercialization strategy involves amassing clinical and economic data to definitively demonstrate that detecting the risk of preterm birth can enable proactive interventions which improve the health of mothers and their babies while at the same time saving substantial health care system costs. Our rigorous, controlled intervention trials, PREVENT-PTB, AVERT PRETERM TRIAL and PRIME, evaluated our test and treat strategy in more than 17,000 patients. We have published two peer-reviewed papers supporting clinically beneficial results from the PREVENT-PTB study and announced positive top-line results in both the AVERT PRETERM TRIAL and PRIME study. Notably, enrollment for the PRIME study was stopped due to efficacy at the interim analysis. We are actively working toward peer-reviewed publications for the AVERT PRETERM TRIAL and PRIME study.
We also work with leading health economists and organizations to build rigorous models that describe how application of the PreTRM test and treat strategy impacts both health and economic outcomes. We work to publish models that provide peer reviewed evidence of the value of our strategy, in the form of meeting presentations and articles.
•Payment and Reimbursement Strategy. Leveraging the demonstrated short- and long-term health and economic benefits of our biomarker approach, our plan is to pursue a variety of payment models, including from integrated systems, self-insured employer markets, large physician practices, and major health insurance payers by working with them to demonstrate the economic benefits of using our biomarker tests. For example, we have a multi-year contract with Elevance Health, one of the largest U.S. health benefits companies, under which Elevance Health agreed to purchase a substantial number of PreTRM tests for pregnant women in their network, and to facilitate commercializing PreTRM testing among its members. The AMA Editorial Board has issued a unique CPT®PLA code for the PreTRM test, which we believe will also help drive payment and coverage decisions for PreTRM testing. In November 2021, this code was priced by the Centers for Medicare & Medicaid Services, or CMS, at $750.
•Broader Market Adoption. For PreTRM, we will seek societal guideline inclusion and to obtain widespread commercial coverage of our biomarker tests from all health care payers as we leverage publications of clinical and economic studies that further demonstrate benefits of the PreTRM test and treat strategy. We anticipate that societal guidelines and payer decisions to cover the test should broadly enable physicians to order testing for their patients. Additionally, we believe that insurance coverage in the United States will help to facilitate coverage of our tests in other countries as we expand internationally in the longer-term. In parallel with our pursuit of broader insurance coverage, we intend to deploy our sales team to address U.S. sales channels to help drive adoption among physician practices.
We envision that our comprehensive approach will enable us to fully characterize one of the most important periods of time in the lives of both women and their babies. We believe that the data and predictions that we develop will ultimately create important information tools and services for a variety of customers, including women, health care workers, insurers, pharmaceutical companies, researchers and related companies. Several future opportunities may be created by comprehensively profiling pregnancy, including, but not limited to:
•additional diagnostic predictors;
•epidemiologic, efficacy and best practice assessment tools to better understand and address critical patient outcomes and disparities across the United States;
•pregnancy educational content development, based on our actual data, for physicians, PAs, nurse practitioners, midwives, regulators, insurers, researchers and health care students; and
•pharmaceutical drug development tools.
We also believe that the work we perform in pregnancy could be leveraged more broadly to address other areas in medicine and health care.
Preterm Birth
Term pregnancy usually lasts between 37 and 42 weeks. Preterm birth is defined as any pregnancy delivering before 37 weeks’ gestation. Preterm delivery includes two major categories: medically indicated preterm birth, where the doctor intervenes because of concerns for the health of the mother and/or the baby, and spontaneous preterm birth where the mother goes into labor spontaneously with no apparent or known pathology.
Of the estimated 140 million annual births globally, approximately 15 million births are preterm. In the United States, there are approximately 3.7 million annual births, and the 2023 March of Dimes Report Card shows that the preterm birth rate is now 10.4% of U.S. births.
Preterm birth remains a leading cause of neonatal morbidity and mortality throughout the world. In the United States, approximately 20,000 annual deaths occur before age one, with prematurity being a major cause. Of the approximately 15 million preterm babies born every year across the globe, about one million die. As a consequence of their preterm birth, many infants require significant medical support in intensive care settings to survive and continue to develop. Preterm birth is also associated with significant long-term disability for many individuals, including learning disabilities, cerebral palsy, chronic respiratory illness, intellectual disability, seizures and impairment of vision and hearing, which can generate significant costs throughout the lives of affected children. The annual U.S. health care costs to manage short- and long-term complications of preterm birth have been estimated to be approximately $25 billion, consisting of direct medical costs incurred during pregnancy, lost productivity due to preterm birth in the perinatal period as well as additional associated longer term medical costs for the mother and child. The estimated average expense per preterm delivery in the United States is approximately $65,000. Earlier preterm births are associated with higher costs due to the greater severity of complications occurring in babies born at earlier gestational ages. Given this, the ability to prolong the gestation period by even one week has the potential for significant savings as shown in the figure below. As a result, the economic benefit of a test that can enable effective interventions to prolong the length of time for a baby to continue developing in utero, even for a short period of time, and to improve neonatal health before delivery is substantial.
Distribution of U.S. Preterm Births and Estimated Average First Year of Life Cost per PTB by Gestational Age at Birth
Unfortunately, traditional methods to predict preterm birth risk fail to identify the great majority of pregnancies that will result in preterm births. Currently, the two most commonly used predictors of preterm birth risk are a woman’s history of prior preterm delivery or a short cervical length measurement found early in pregnancy. It is estimated that only about 1 out of 6 singleton spontaneous preterm births can be detected proactively with these clinical methods. The great majority of
singleton preterm births only become apparent when the woman goes into labor and delivers, at which point proactive management options are no longer possible. Therefore, the ability to identify the great majority of women who will, in fact, deliver prematurely, and thus be able to more proactively manage their risk, represents a significant unmet medical need and offers a pivotal opportunity to make a positive difference for the mother and the baby.
Proactive interventions to address higher preterm birth risk may include more frequent contact with the patient, additional clinical visits, more intensive education and monitoring of the patient during pregnancy, prophylactic administration of progesterone or anti-inflammatory medications, heightened awareness of impending delivery and reacting more promptly to changes indicative of preterm birth as the pregnancy progresses.
The PreTRM Test — Our Solution for Preterm Birth
Utilizing our product discovery, development and commercialization approach, and in view of these stark realities of preterm birth, we focused our first development and commercialization efforts on addressing preterm birth. Our first product, the PreTRM test, is the only broadly validated, commercially available blood-based biomarker test to accurately predict the risk of spontaneous preterm birth. The PreTRM test is a non-invasive blood test given to a pregnant woman, carrying a single fetus, during weeks 18 through 20 of gestation. The specimen analyzed in the PreTRM test is drawn once in single fetus, or singleton, pregnancies where there is no evidence of significant fetal anomalies by non-invasive pre-natal genetic screening, or NIPS, or ultrasound, and the women tested are not taking progesterone. The blood specimen is analyzed in our CLIA-approved clinical laboratory using our high throughput mass spectrometry technology. Once the laboratory analysis is completed, a risk report is generated from our validated algorithm and the results are transmitted to the ordering clinician. The PreTRM test provides an accurate prediction of the expectant mother’s individualized risk, expressed as a percentage, of delivering spontaneously before 37 weeks’ gestation, as well as her relative risk compared to the average population risk. The great majority of singleton preterm births are spontaneous, where the mother goes into labor and delivers without any apparent known pathology.
The PreTRM test combines the ratio of insulin-like growth factor-binding protein 4, or IBP4, to sex hormone-binding globulin, or SHBG, with a woman’s height and weight to predict the risk of spontaneous preterm birth. These protein biomarkers have been extensively validated in multiple maternal fetal medicine centers located in the United States, Europe, Asia and Africa. In addition, we continue to build on our existing data to further demonstrate the clinical and economic benefits of intervening based on PreTRM test results. The PreTRM test accuracy has been rigorously assessed and validated in our PAPR study involving 5,501 women in 11 obstetric centers across the United States. Our completed PAPR study validated the biomarker signature which is highly predictive of spontaneous preterm birth risk. The performance of the PreTRM test biomarkers was replicated in a second independent large prospective U.S. study, TREETOP, supporting that the IBP4 to SHBG predictor can be used to accurately risk-stratify patients for implementation of preterm birth preventive strategies and direct patients to appropriate levels of care. The ability to accurately risk-stratify is critical for enabling precision care management. We and our collaborators are also conducting or have completed three prospective controlled intervention studies — The Prediction and Prevention of Preterm Birth, or PREVENT-PTB, study, or PREVENT-PTB, the Serum Assessment of Preterm Birth Outcomes Compared to Historical Controls, or AVERT PRETERM TRIAL and Prematurity Risk Assessment Combined With Clinical Interventions for Improving Neonatal outcoMEs, or PRIME — to demonstrate the value of identifying higher risk pregnancies coupled with proactive interventions to improve the well-being of mothers and newborns.
We believe our comprehensive approach to build evidence for our PreTRM test addresses key elements payers require in order to reimburse testing, including:
•analytical validation of the testing platform, or measurement validity;
•clinical validation, or test validity;
•clinical utility of using validated predictions, or positive health benefit; and
•economic utility, or cost effectiveness and health care savings.
Underscoring the benefits of the PreTRM test and treat strategy, the clinical and economic utility of the PreTRM test administered mid-pregnancy has been published by respected independent health economists in a leading maternal fetal medicine journal.
The strength of the data from our studies of the PreTRM test has enabled us to pursue an innovative and accelerated approach to commercialization. Elevance Health, whose health plans cover more than 10% of U.S. pregnancies annually, agreed to pay for our PreTRM test for eligible pregnant members as part of a multi-year contract. The collaboration also enables us to generate more data to demonstrate the value of the PreTRM test and treat approach across diverse patient populations within Elevance Health’s insurance plans.
Biomarker Discovery and Clinical Validation of the PreTRM Test
Adherence to National Academy of Medicine Guidelines
We rigorously adhere to authoritative NAM guidelines published in 2012 for developing and validating multi-omics predictions and applying important principles to address adverse conditions that arise in pregnancy. The guidelines specify three phases of work to be performed in non-overlapping sets of specimens:
Discovery Phase. A set of specimens from patients whose outcomes are known are analyzed in the lab to find biomarker differences between individuals with an adverse outcome versus individuals without that particular outcome (e.g., pregnancies that deliver preterm versus term pregnancies). Algorithms are built on high performing predictions that can be tested in the next phase.
Verification Phase. High-performing predictive algorithms selected from discovery work are pre-specified and applied to a completely independent set of non-overlapping specimens, with the laboratory being blinded to the outcomes. The performance of the algorithms is either independently verified, or confirmed, by an external statistician, who ranks the algorithms according to predictive accuracy. Once verified, highest performing algorithms are locked down in the form of optimized tests that can be validated in final validation phases before commercialization.
Validation Phase. In a third, entirely independent set of non-overlapping specimens, the laboratory measurements are performed, and the laboratory is blinded to patient outcomes. The laboratory data are time-stamped and are transferred to an external statistician, who applies the pre-specified algorithm to the laboratory measurements and independently validates the performance of the test by breaking the blind. At this point, a prediction that has been independently and rigorously validated can be used for clinical decision-making in trials and/or commercialization.
PAPR Study
The biomarkers used in the PreTRM test have demonstrated strong clinical performance in accurately predicting women at risk of preterm birth across diverse patient populations in the United States, Europe, Asia and Africa. The initial discovery, verification and validation of our spontaneous preterm birth biomarker risk predictor was performed in the 5,501 patient Proteomic Assessment of Preterm Risk, or PAPR, study.
The PAPR study was initiated in April 2011 and the last observed birth occurred in February 2014. The study was designed to discover, verify and validate biomarkers and clinical variables that accurately predict the risk of spontaneous preterm birth. We measured and evaluated protein expression of thousands of distinct proteins, using our proprietary proteomic workflow, by their levels in maternal serum to assess their effectiveness as predictors of spontaneous preterm birth early in pregnancy before symptoms occur. This analysis showed strong predictive power of a specific combination of two proteins, IBP4 and SHBG, coupled with clinical variables consisting of a woman’s height and weight, which we developed into a proprietary predictive algorithm that forms the basis of the PreTRM test. These results of the PAPR study were reported in detail at Saade et al., Am. J. Obstet. Gynecol. (2016) 214:633. Samples from PAPR subjects consented for biobanking are used to develop predictors and products for other pregnancy complications.
TREETOP Study
Our second large clinical validation study, A MulTicenteR AssEssmEnt of a SponTaneOus Preterm Birth Predictor, or TREETOP, enrolled patients beginning in October 2016 with the last delivery occurring in May 2019. The TREETOP study enrolled 5,011 pregnant women from 18 sites across the United States, and validated a PreTRM test risk threshold to statistically stratify higher versus lower risk patients based on a pre-specification of the threshold from PAPR data and by applying it to specimens in this cohort. The validated threshold of 15%, twice the average population risk of spontaneous preterm birth, was demonstrated to statistically separate patients at higher versus lower risk of preterm delivery based on the PreTRM test results. This is the risk threshold for interventional actions to be taken in the PRIME prospective
intervention trial that was initiated in 2020. These results were reported in detail at Burchard et al., J. Clin. Med. (2021) 10:5088.
Given the large body of evidence generated from PAPR and our other collaborative biomarker studies, the TREETOP specimens were randomized into two cohorts:
•a first patient cohort of 847 specimens to validate certain pre-specified predictions originating from our earlier PAPR study work, and to verify new potentially enhanced predictions that could be validated later on the specimens of the remaining unanalyzed cohort of patients; and
•a second cohort of remaining specimens was held in reserve to validate, in the future, a number of potentially enhanced predictions that may eventually be incorporated into our commercially available testing as we build our pipeline of adverse pregnancy outcome predictions.
Thus, PAPR and TREETOP together encompass a powerful resource of specimens and clinical data from thousands of pregnant women collected over an eight-year period to characterize what takes place biologically in pregnancy. Both PAPR and TREETOP enrolled a large number of women who were not known to be at risk of preterm birth based on other identified clinical factors, and as such, were not already covered by professional society guidelines addressing the need for risk stratification and guidance of treatment. We believe further analysis of the specimens and data from these studies may provide a deep view into the outcomes of diverse singleton pregnancies across the United States and prediction of these outcomes. For example, we used some of these specimens to improve the predictive performance of the PreTRM test and expand the blood draw window to a three-week period.
Our Prospective Intervention Studies — Demonstrating the Benefits of the PreTRM Test and Treat Strategy
Following the validation of predictors for spontaneous preterm birth, we set out to demonstrate the value of identifying higher-risk pregnancies coupled with proactive interventions to improve the well-being of mothers and newborns. We have worked with respected collaborators to conduct three prospective intervention studies in order to demonstrate the clinical utility and economic value of the PreTRM test and treat approach.
PREVENT-PTB Study
The Prediction and Prevention of Preterm Birth, or PREVENT-PTB, study (Clinical trials identifier: NCT03530332) was a prospective randomized controlled intervention study conducted at Intermountain Healthcare in Salt Lake City, Utah. The PREVENT-PTB study enrolled a total of 1,208 patients to evaluate the health and economics impact of applying the PreTRM test.
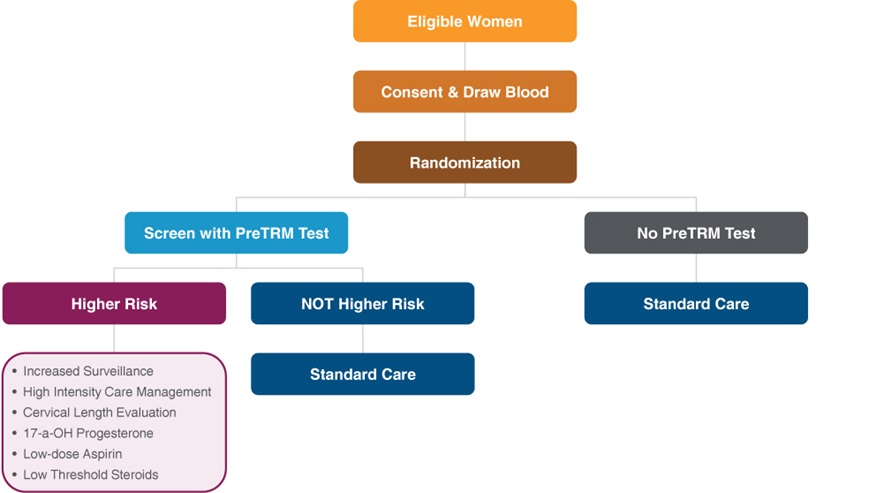
In the PREVENT-PTB trial, women enrolled were randomized 1:1 to either the screened or control group. Women in the screened group received the PreTRM test, and those at higher risk of preterm birth according to the test result were offered a menu of proactive interventions. These included care management (i.e. weekly contact with a care management nurse, preterm prevention clinic visits, evaluation of signs and symptoms of prematurity, education, cervical length monitoring) and medications (17-α-hydroxyprogesterone caproate, low-dose aspirin and the administration of corticosteroid treatment at a lower threshold if patients indicated clinical signs or symptoms of imminent delivery). Patients in the screened group that were found not to be at higher risk by the PreTRM test and those in the control group received standard obstetrical care. The diagram below illustrates the study design for PREVENT-PTB:
Study Design of PREVENT-PTB
The PREVENT-PTB results were published on August 16, 2021 in the American Journal of Perinatology. The key reported findings were:
•Hospital and NICU length-of-stay reduced by more than 70% in preterm infants;
•Severe neonatal morbidity or death was reduced by 66% across infants affected by complications of prematurity;
•Significantly faster discharge rates of preterm deliveries from the NICU; and
•Observed 23-80% reduction in preterm delivery rates occurring before 37, 35, and 32 weeks of pregnancy, even though the study was not statistically powered to definitively answer whether rate reductions were possible.
AVERT PRETERM TRIAL
The Serum Assessment of Preterm Birth Outcomes Compared to Historical Controls, or AVERT PRETERM TRIAL (Clinical trials identifier: NCT03151330), was a large prospective, historically-controlled intervention trial conducted at ChristianaCare in Newark, Delaware. The purpose of the study was to evaluate the impact on health and economics by applying the PreTRM test to screen pregnant women for risk of spontaneous preterm delivery and to proactively intervene in individuals who were shown by the PreTRM test to be at higher risk of sPTB. Those deemed by the test to be at lower risk received standard care, as did the historical control population. As in the PREVENT-PTB study, interventions in the higher-risk group included care management (closer monitoring by their clinicians and case management nurses) and medications (e.g. vaginal progesterone, low-dose aspirin). The two co-primary endpoints were reduction in total neonatal hospital length of stay and improvement in composite neonatal morbidity and mortality in the PreTRM-screened group versus the historical control group, which did not have a PreTRM test.
Design of the AVERT PRETERM TRIAL
Health and economic outcomes of the screened group were compared with those of the historical control arm. Due to the COVID-19 pandemic, trial enrollment of the prospective arm was stopped in March 2020. On February 15, 2023, we announced that both co-primary outcomes—reduction of severe neonatal morbidity or neonatal death; and decreased length of neonatal hospital stay—met their endpoints, and the improvements in outcome with a PreTRM test-and-treat approach were statistically significant. Detailed results of the AVERT PRETERM TRIAL analysis are being prepared for publication in a peer-reviewed journal.
PRIME Study
In collaboration with Elevance Health, we are conducting Prematurity Risk Assessment Combined With Clinical Interventions for Improving Neonatal outcoMEs, or PRIME (Clinical trials identifier: NCT04301518), study, which is a prospective randomized controlled study of up to 6,500 enrolled pregnancies in 15 respected maternal fetal medicine centers. We began enrollment in November 2020. In December 2023, we announced that the Data Safety Monitoring Board, or DSMB, overseeing our PRIME study recommended stopping enrollment due to efficacy, reporting that either co-primary endpoints, neonatal hospital length of stay and composite neonatal morbidity and mortality, met the stopping criteria for statistical significance at the pre-planned interim analysis. We adopted the DSMB’s recommendation and stopped PRIME study enrollment to focus on analyzing and reporting the available data. A manuscript reporting study results, including top-line and exploratory analyses, is being prepared for submission and peer review.
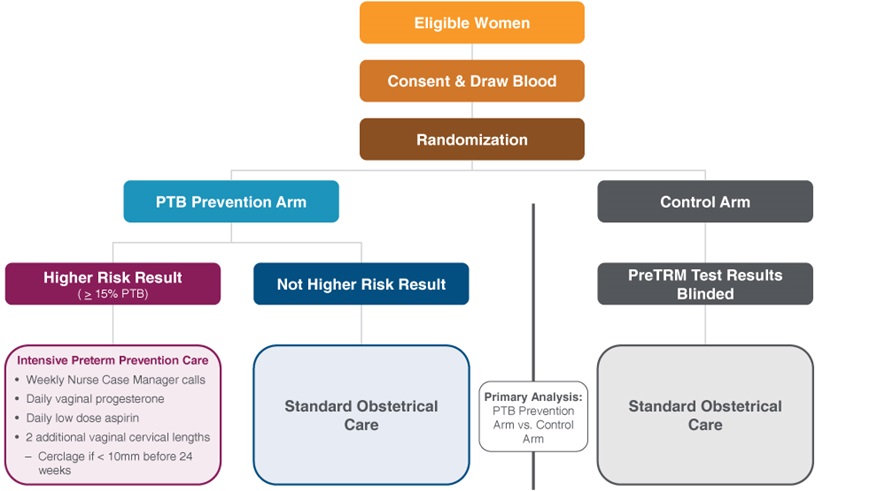
After enrollment, subjects had a blood specimen collected once during either week 19 or 20 of pregnancy (after June 28, 2022, the collection window was expanded to include the 18th week of pregnancy). Prospectively enrolled pregnant women were randomized 1:1 to either a screened arm, called the PTB Prevention arm, or a control arm that received standard obstetrical care. Only subjects randomized to the PTB Prevention arm received the results of the PreTRM test. Those women randomized to the PTB Prevention arm received either routine standard care pregnancy management or a multimodal intervention protocol reserved for higher risk pregnancies based on the results of the PreTRM test. The design of the PRIME study is illustrated below.
Design of the PRIME Study
In the PTB Prevention arm, PreTRM test results were reported to the subject, the study investigator and the subject’s primary pregnancy care provider. A woman with a reported “Higher Risk” test result, at or above the 15% threshold (which is equivalent to more than a doubling of average population risk of spontaneous preterm delivery less than 37 weeks’ gestation), received multiple interventions, including weekly nurse case management contact, daily vaginal progesterone, daily low dose aspirin and additional vaginal ultrasound cervical length determinations, with cerclage considered for cervical lengths less than 10 millimeters. Subjects in the “Not Higher Risk” group received standard obstetrical care for the duration of pregnancy through hospital discharge.
Major perinatal outcomes to be evaluated in each group include length of NICU and total hospital stay, measures of neonatal health, NICU preterm costs and preterm delivery rates. All subjects will be followed through the duration of the pregnancy and delivery, and neonates will be followed until initial hospital discharge to assess the course of pregnancy, labor and any related maternal or fetal complications. Readmission of infants will also be assessed at 180 days, 1 year and 3 years of life using the Elevance Health/Carelon Research Integrated Research Database to evaluate longer-term outcomes and costs associated with preterm delivery.
Other Relevant Studies and Publications
Clinical and Economic Evaluation of the PreTRM Test
This study modeled the clinical and economic impact of the PreTRM test for patients in the TREETOP study using actual prospectively determined test results. The model predicted improvements in neonatal and maternal hospital length of stay by 19% (p = .029) and 8.5% (p = .001), respectively, compared with standard care; neonatal costs’ point estimate reductions of 16% (p = .098); and a reduction in moderate-to-severe neonatal morbidity/mortality by 29% (p = .025). In a manuscript published in December 2022, the authors concluded that the modeled evaluation of a biomarker-based test-and-treat strategy in a diverse population predicts clinically and economically meaningful improvements in neonatal and maternal outcomes (Burchard et al. J. Med. Econ. 2022 Jan-Dec;25(1):1255-1266.)
Care Management as a Component of Obstetric Care
This review investigated the obstetrical benefit of care management, defined as specialty clinics, social services, coordination of specialty services such as nutrition counseling, home visits or frequent phone calls by specially trained personnel, and other elements. Evidence was found for consistent reductions or trends toward reductions in preterm birth with care management, particularly among individuals with high a priori risk of preterm birth across systematic reviews, meta-analyses, and randomized controlled studies. The authors concluded that care management has substantial potential to
improve the environmental, behavioral, social, and psychological factors with patients at risk of preterm birth (Garite and Manuck. Am. J. Obstet. Gynecol. 2022 Sep 19:S0002-9378(22)00746-3).
Carelon Research/Elevance Health and Economic Study
Carelon Research, a subsidiary of Elevance Health, conducted an insurance claims data analysis on the cost-effectiveness of screening more than 40,000 mothers and babies within Elevance Health’s commercially insured membership. The model evaluated the cost impact to be expected from screening with the PreTRM test, and from then providing a bundle of interventions to PreTRM-higher risk patients as compared to the effect of standard care without a PreTRM test. The model predicted that these interventions would result in:
•a 20% reduction in preterm birth before 37 weeks’ gestation;
•$1,608 in gross savings per pregnant woman tested (accounting for all costs except that of a $745 list price cost modeled for the PreTRM test);
•a 10% reduction in neonatal intensive care admissions;
•a 7% reduction in overall hospital length-of-stay; and
•a 33% reduction in births at less than 32 weeks’ gestation.
The authors concluded that the PreTRM test and treat strategy demonstrated cost savings across a variety of reasonable assumptions and scenarios examined. An abstract reporting these results was presented at the 2021 International Society for Pharmacoeconomics and Outcomes health economic conference on May 18, 2021, and a manuscript was published on the results on September 14, 2021 in the journal ClinicoEconomics and Outcomes Research. Grabner et al., Cost-Effectiveness of a Proteomic Test for Preterm Birth Prediction; Clinicoecon. Outcomes Res. (2021) 13:809-820.
The Vietnam Preterm Birth Biomarker (PBB) Study
We have continued our commitment to bring our technology to ex-US geographies and low- and middle-income settings through Bill & Melinda Gates Foundation funded research by validating the PreTRM test in a large cohort in Vietnam. On March 13, 2024, the manuscript entitled: Validating the ratio of insulin like growth factor binding protein 4 to sex hormone binding globulin as a prognostic predictor of preterm birth in Viet Nam: a case-cohort study, was accepted for publication in The Journal of Maternal-Fetal & Neonatal Medicine.
Product Pipeline
While we have leveraged our technology platform to currently pursue the development and commercialization of the PreTRM test, we believe our technology platform has broad applicability across a wide array of pregnancy-related conditions. We and our clinical trial collaborators are also continuing to conduct analyses by combining biobank data from the PAPR and TREETOP studies, to provide new insights into the predictive capabilities of the PreTRM test and other predictive biomarker algorithms. We are discovering, developing and validating a broad portfolio of product candidates including those focused on the conditions listed below.
When we refer to “discovering, developing and validating” our product candidates, we are referring to the three phases of work for development of predictive tests as published in the NAM guidelines, as summarized below.
In the “discovery” phase, we analyze a set of biologic specimens from patients whose pregnancy outcomes are already known to find biomarker differences between individuals who had an adverse pregnancy outcome versus individuals who did not have an adverse pregnancy outcome (e.g., pregnancies that delivered preterm versus pregnancies that lasted to term). We then build predictive algorithms, based on high performing predictions, to be tested in the next phase.
In the “verification” phase, we apply the high performing predictive algorithms selected during the discovery phase to a completely independent set of new biologic specimens that were not tested during the discovery phase. An independent, external statistician then verifies, or confirms, the performance of the algorithms, and ranks them according to predictive accuracy. Once they are verified through this process, the highest performing algorithms are “locked down” in the form of optimized tests that can be validated in a final phase, prior to commercialization.
In the “validation” phase, a third, entirely independent set of biologic specimens that were not tested during either the discovery phase or the verification phase are tested in a laboratory, with the laboratory blinded to patient outcomes. The laboratory data are time-stamped and are transferred to an external statistician, who applies the pre-specified algorithms to the laboratory measurements and independently validates the performance of the test by breaking the blind. At this point, a prediction that has been independently and rigorously validated can be used for clinical decision-making in trials and/or commercialization.
Molecular Time-to-Birth
Problem and Need. We have already developed a high performing biomarker signature in our PreTRM test for spontaneous preterm birth risk. For a pregnant woman who is not at higher risk of preterm birth by our PreTRM test, she would typically like to know how much time is remaining in her pregnancy until delivery. Unfortunately, current methods for predicting the length of gestation, including due date prediction from last menstrual period and ultrasound dating based on fetal measurements early in pregnancy, lack precision and provide inaccurate dating as to when delivery will occur. We have identified biomarker signatures that predict the time remaining in a pregnancy with greater accuracy than is available from current methods.
Objective for a Biomarker Test. Our objective is to develop a more accurate time-to-birth prediction for women not at higher risk of PTB. We believe this will be of great interest to pregnant women as a consumer test that may serve as an aid to decision-making for travel, work, vacation planning and other life-scheduling decisions.
Development Status. Using our proprietary biobanks and proteomics platform, we have discovered and verified biomarkers with superior time-to-birth predictive performance, as compared to current dating methods. We have developed the ability to determine more precisely how much time is remaining in a woman’s pregnancy based on her individual biology at the time of her blood draw. We are exploring the optimal commercialization strategy of a molecular time-to-birth predictor and plan to publish its performance data in due course.
Predictive Analytics
Problem and Need. As we have accumulated tens of thousands of highly curated pregnancies in our databases, the application of machine learning has opened the potential for predictive pregnancy analytics that give insight on many critical aspects of pregnancy that are relevant to both the mother (e.g. planning, expectations, education) and her physician (e.g. risk assessment, management planning).
Objective for a Predictive Analytics Tool. We are working to develop a predictive analytics tool that can be used in combination with our clinical tests, or on its own, as a tool to understand various features and conditions of pregnancy, for both the benefit of the mother and physician.
Development Status. We have completed discovery work and are now performing market assessments of a prototype.
Pregnancy Risk Prediction Panel
Condition. Up to 31% of pregnancies will develop a significant complication. Furthermore, traditional clinical risk factors miss two-thirds of these complications. The intended use of the pregnancy risk prediction panel is to identify those pregnancies at high risk of developing a significant complication so they can be triaged to enhanced management and further assessment.
Development Status. Discovery and verification work are complete, as well as a robust initial market assessment of physicians, patients, and payers.
Preeclampsia
Condition. Preeclampsia, estimated to affect 5% - 8% of pregnancies in the United States, is a complication characterized by high blood pressure and signs of damage to one or more organs, including liver, brain and kidneys, and may also have adverse effects on blood coagulation. Preeclampsia usually begins after 20 weeks of pregnancy in women whose blood pressure had been normal, but it can also arise earlier in pregnancies. Left untreated, preeclampsia can lead to serious, even fatal, complications for both the mother and baby. Once a pregnant woman is diagnosed with preeclampsia, a common treatment is to deliver the baby; however, if the delivery occurs before the infant reaches term (preterm
preeclampsia), complications of preterm birth can ensue and clinical decisions are challenged by weighing the risk to the mother of continuing the pregnancy versus the risks to the baby associated with early delivery. We believe that a biomarker test to better identify women who are at higher risk of preterm preeclampsia earlier in pregnancy could lead to better management of this serious condition. It is estimated that the U.S. annual cost of preeclampsia is approximately $5 billion.
Objective for a Biomarker Test. We are working to develop a protein biomarker test that can identify women at higher risk of developing preterm preeclampsia as a means to enable earlier proactive interventions to mitigate the complications that occur as a result of this condition. We believe that such interventions could also prevent preeclampsia in certain patients, which has the potential of lowering the long-term risk of cardiovascular disease and stroke that occur later in life in women who suffer preeclampsia. There is also potential for a predictive biomarker test to inform therapeutic development to address this condition.
Development Status. We have completed discovery, verification and validation using our proprietary biobanks of several preterm preeclampsia biomarker predictors, some of which have been published. Some of these predictions include the use of our PreTRM test biomarkers as well as others. We are in the process of selecting the final predictor and the optimal commercialization strategy.
Growth Restriction
Condition. Fetal growth restriction, or FGR, is estimated to affect as many as approximately 3%-7% of pregnancies worldwide. There are immediate consequences of FGR, including fetal challenges in withstanding the stresses of vaginal delivery, decreased oxygen levels and brain injury, hypoglycemia (low blood sugar), lower resistance to infection, difficulty in maintaining body temperature and abnormally high red blood cell counts. In the longer term, infants can have neurodevelopment issues, metabolic and cardiovascular complications.
Objective for a Biomarker Test for FGR. By identifying molecular events that precede measurable changes in fetal size, we aim to address the placental dysfunction and other growth restriction etiologies that lead to fetal growth restriction and thereby enable earlier proactive interventions.
Development Status. We have discovered placental dysfunction biomarkers as a first step to predicting fetal growth restriction. We are working to discover additional biomarkers that illustrate expression differences in normal and growth-restricted pregnancies. We believe that this work could lead to improved detection of FGR pregnancies earlier and may lead to proactive interventions to better address this problem. Verification and validation phases and publication of our findings, based on the NAM guidelines described above, will be required before such testing can be commercialized.
Other Potential Products
Gestational Diabetes Mellitus
Condition. Gestational diabetes mellitus, or GDM, is characterized by high blood sugar levels, or hyperglycemia, during pregnancy in a woman who was not diabetic before her pregnancy. GDM is estimated to affect approximately 10% of pregnancies and cost $1.6 billion annually in the United States as a result of short- and long-term maternal and child complications. GDM increases the risk of preeclampsia, depression, and the need for Caesarean sections. Babies born to mothers with poorly treated GDM are at increased risk of being too large, having low blood sugar after birth, and jaundice. If untreated, GDM can also result in stillbirth. Children born from mothers with GDM are also at risk of being overweight and developing type 2 diabetes. We believe that knowing who is at high risk of GDM earlier in pregnancy would be of great benefit given that interventions could significantly reduce the adverse effects of this condition. Current methods for identifying GDM in most patients typically take place between 24-26 weeks’ gestation, missing opportunities to allow such women to receive proactive interventions earlier in pregnancy that may be effective in preventing or mitigating GDM.
Objective for a Biomarker Test. Our goal is to develop a blood-based biomarker test that can identify earlier in pregnancy which women are likely to develop GDM. We believe that such information will enable earlier interventions to mitigate risks and help focus resources on higher risk pregnancies as a means to improve the health of mothers and babies.
Development Status. We have discovered and verified high performing biomarker prediction of GDM by applying our proteomics platform technologies to specimens from our PAPR and TREETOP biobanks. We plan on further verifying and ultimately validating a GDM predictor and publishing its performance data prior to making it available commercially, based on the NAM guidelines described above.
Stillbirth
Condition. Stillbirth is a heartbreaking and tragic outcome, with a reported incidence of 5.7 per 1,000 pregnancies in the United States. Stillbirth is typically defined as fetal loss occurring after 20 weeks’ gestation. Causes of stillbirth include placental or umbilical cord problems, preeclampsia, lupus, clotting disorders, lifestyle choices, and infection, among others. Approximately one-third of U.S. stillbirth cases occur without any known cause.
Objective for a Biomarker Test for Stillbirth. Our goal is to discover biomarker expression changes that occur early during pregnancy that are highly predictive of changes taking place in the mother and/or the fetus that increase the risks of stillbirth, so that appropriate interventional strategies can be developed to address this condition. Given that our vision is to comprehensively profile the biology of pregnancy by leveraging our platform technologies to characterize disruption of normal developmental biology in both the mother and the fetus, we believe that there is a significant opportunity to improve earlier detection and the potential to develop targeted interventions to better address this serious problem.
Development Status. We have developed the ability to measure the expression of hundreds of proteins by our advanced mass spectrometry proteomic technology. These proteins are members of key biochemical proteomic pregnancy signaling pathways, including pathways that are operative in stillbirth. As we increase the density of proteins characterized in future discovery work, we believe that further characterization of pregnancy and key proteomic expression factors in stillbirths vs. normal pregnancies is a promising area for further discovery, verification and validation of high performing biomarkers predictors with potential to improve detection and enable new interventions for stillbirth. Finally, we note that development for prediction of other adverse outcomes (e.g., growth restriction) has the potential to reduce stillbirth.
Postpartum Depression
Condition. There are hormonal, physiological and psychological changes that occur in women both during and after pregnancy. Postpartum depression is a severe form of clinical depression related to pregnancy and childbirth, affecting approximately 15% of women during the year following delivery of a child. By contrast, the “baby blues” is a transient, well-known phenomenon that typically resolves on its own. The annual U.S. economic burden of postpartum depression is estimated to be approximately $2.4 billion. We believe that a biomarker test for postpartum depression is another area are where our platform can be beneficially applied. We believe that early identification of such pregnancies will enable a number of approaches that may prevent or mitigate the severity of this common condition, and that this information may also facilitate drug discovery.
Objective for a Biomarker Test for Postpartum Depression. Our objective is to leverage our understanding of key pregnancy, pathways gained through the application of our advanced proteomic technologies and bioinformatics, to develop further insights for early identification of pregnancies that are destined to develop postpartum depression.
Development Status. In our discovery efforts, we have discovered protein expression patterns in hormone signaling pathways and other pathways of pregnancy that we believe may be operative in the development of postpartum depression. We are working to increase the coverage of biochemical signaling pathways and expression patterns related to postpartum depression in our protein expression database, which we believe will enable the development of a high performing predictor to address this area.
Timing of Pipeline Developments
In the development of high-performing biomarker signatures, the timing of when to move from the discovery phase to the verification phase to the validation phase, based on the NAM guidelines described above, is entirely dependent on the performance data. There are also the additional requirements to analytically validate the particular components measured in biomarker tests by our laboratory and to build the informatics and automation for integrating all components into new testing processes. Given the uncertainties in reliably predicting timing for these phases and additional requirements, we estimate that the timing for our next new commercially available product is a matter of months or years. We will only advance our programs from one stage to the next if we believe that they qualify for advancement pursuant to the NAM guidelines described above. We believe that additional capital required to do this work could help to accelerate the progress on our comprehensive pregnancy pipeline.
Commercialization
The beginning of life and end of life are widely recognized to be costly periods for health care services in the human life cycle. Health care insurers characterize preterm birth as an exceptionally costly condition, and a number of them develop data and models that underscore the economic impact of preterm births. Given the substantial economic benefits promised by the use of the PreTRM test, we are pursuing payment for the PreTRM test by integrated systems, large physician practices, and major health insurance payers. We are collaborating with Elevance Health in the PRIME study to generate rigorous data across at least 15 centers across the United States. Elevance Health is paying us for PreTRM testing done as a part of that study at a specified rate per test, pursuant to a Laboratory Services Agreement described under “— Material Agreements” below. Furthermore, we have entered into a commercial collaboration agreement with Elevance Health to introduce PreTRM testing into its various health plans.
Generating publications and scientific presentations is a core pillar of our market awareness strategy and is important for establishing validity and utility of new products in the life sciences community. We plan to work closely with maternal fetal medicine experts, payers and key opinion leaders to generate clear use-cases, as well as peer-reviewed publications that illustrate our product performance claims and value proposition. We have worked and continue to work with more than 60 investigators world-wide. In addition, we plan to increase awareness by developing and deploying online and in-person training and educational tools that explain the PreTRM test and our proteomics and bioinformatics platform in easy-to-access, easy-to-understand and credible, scientifically rigorous ways.
When the evidence base supporting our products, payment trends, medical society and provider adoption, and general market conditions warrant, we expect to increase our investment in field and inside sales, marketing, customer service, and managed care personnel. We anticipate that our sales team will promote our products in the United States, which may include a targeted focus on OB/GYNs and maternal-fetal medicine providers in certain key markets and segments (e.g., integrated systems, large physician practices). Full commercialization of clinical tests may also require an experienced market access team to secure contracts with commercial and governmental payers, and each of our products may benefit from a multi-faceted digital marketing platform to scale consumer awareness and engagement. We are also evaluating the expansion of our business internationally, with the PreTRM test representing one potential avenue for expansion.
Our Clinical Laboratory Characteristics
Our PreTRM testing laboratory is based in Salt Lake City, Utah. We operate under federal regulations as a CLIA-certified laboratory, and we hold all required state licenses. We undergo regular inspections from federal and state regulatory authorities, and our laboratory is accredited by the College of American Pathologists, or CAP.
We have optimized our mass spectrometry-based proteomics workflow to be analytically validated to produce accurate and precise patient results. To meet the demands of the large intended use population of the PreTRM test, we have validated an ambient specimen collection and shipping process that removes the need to ship specimens under frozen conditions using dry ice. Additionally, we are further developing state-of-the-art affinity-capture mass spectrometry, or AC-MS, process. This higher through-put and lower-cost improvement to our current workflow utilizes custom monoclonal antibodies and magnetic beads. Affinity capture of our PreTRM test analytes using magnetic beads coated with antibodies is amenable to automated liquid handling robots using 96 or 384 well plates. Moreover, the AC-MS process results in a large decrease in the complexity of patient serum specimens in a single highly parallel and multiplexed step, which translates to shorter mass spectrometry processing times. We believe the AC-MS process can be leveraged to enable a many-fold increase in capacity and significantly decrease turn-around time and cost of goods sold. We are also developing immunoassays, some of which may be able to incorporate the custom antibodies developed for the AC-MS process. AC-MS and immunoassay versions of our testing products may be suitable for our current ambient process and other lower-cost specimen collection and shipping devices in the future.
Material Agreements
Elevance Health Commercial Collaboration Agreement
In February 2021, we entered into a commercial collaboration agreement with Elevance Health, or the Commercial Collaboration Agreement, relating to the commercialization of the PreTRM test.
Under this agreement, we agreed to provide PreTRM tests to eligible individuals enrolled in, or serviced or covered by, the health insurance products of Elevance Health. We also agreed to develop a sales, marketing, and customer service
program, and to provide training and marketing to duly licensed physicians specializing in obstetrics and gynecology or family medicine, or licensed nurse midwives, at the reasonable request of Elevance Health. Pursuant to the agreement, Elevance Health agreed to purchase a specified minimum number of tests from us for each of the first three years of the term of the agreement. Additionally, Elevance Health agreed to pay us a specified minimum amount per year for the first three years of the term of the agreement.
Elevance Health has been participating in our PRIME study, and at the conclusion of the PRIME study, under the Commercial Collaboration Agreement, the parties agreed to use commercially reasonable efforts to enter into Elevance Health’s standard lab provider agreement. Unless earlier terminated due to breach, the Commercial Collaboration Agreement will remain in effect until the later of (a) the third anniversary of the effective date or (b) the date on which Elevance Health has purchased a fixed number of PreTRM tests as agreed by the parties.
Elevance Health Laboratory Services Agreement
Effective in November 2020, we entered into a laboratory services agreement with Elevance Health, or the Laboratory Services Agreement, relating to our provision of PreTRM tests and related services during the course of the PRIME study.
Under this agreement, we agreed to provide clinical laboratory services as requested by participating physicians and other health care professionals, and written reports to those physicians and professionals of the results of the services performed in accordance with the PRIME study. Elevance Health agreed to collaborate with us on the conduct of the PRIME study, and will pay us a specified amount per test up to a specified maximum number of tests.
Unless earlier terminated due to breach, the Laboratory Services Agreement will remain in effect until the conclusion of the PRIME study, and it may thereafter be extended for additional terms of one year upon mutual agreement of the parties.
Competition
The life science industry, including companies engaged in molecular diagnostics and proteomics, is characterized by rapidly advancing technologies, intense competition, substantial resources devoted to securing strong intellectual property protection and a focus on developing innovative, proprietary products. To our knowledge, however, there have been few successful efforts by others to date to discover, verify and validate prognostic biomarker tests to predict conditions of pregnancy, and we are aware of no competitors that have discovered, verified and broadly validated a blood-based biomarker test to predict a pregnant woman’s risk of a spontaneous preterm birth. We therefore believe that our PreTRM test has the benefit of strong first-to-market positioning and validated performance as we pursue our commercialization efforts. In addition, we believe that our proprietary technology platform, including our extensive biobanks, advanced mass spectrometry approaches and bioinformatics capabilities, provides us with valuable competitive assets to utilize in discovering and developing other products and services for pregnancy conditions, several of which are already in our pipeline. Coupled with the experience and expertise of our management and scientific teams, we believe we possess meaningful potential to compete in developing and commercializing important products to improve the pregnancy experience and the health of mothers and babies.
Notwithstanding the foregoing advantages, given the potential market opportunity represented by the PreTRM test and other pregnancy-related products and services that we may develop, we expect competition to emerge and intensify in the coming years, with one or more competitive offerings resulting from competitors’ efforts. Competing products may arise from various sources, including molecular diagnostic companies, clinical laboratory companies, life sciences tool companies, third-party service providers, academic research institutions, governmental agencies and public and private research institutions. From time to time, results of early biomarker discovery work are published in scientific literature. These publications are demonstrative of interest in the field, but they have so far typically lacked evidence of strict adherence to the NAM guidelines for multi-omics prediction development and have not achieved rigorous validation of predictions of interest.
Many of the potential competitors that may emerge, either alone or with their collaborators, may have significantly greater resources, established presence in the market, expertise in research and development and greater experience in laboratory operations, obtaining regulatory approvals, gaining reimbursement and commercializing approved products than we do. These competitors are also expected to compete with us in recruiting and retaining qualified scientific, sales, marketing and management personnel, conducting clinical studies, publishing scientific research and acquiring technologies that may be complementary to, or necessary for, the ongoing robustness of our discovery, development and
commercialization efforts. Other smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. Additional mergers and acquisitions may result in even more resources being concentrated in our competitors.
Sales and Marketing
As we continue to engage with payers, self-insured employers, health systems, and other payment models using our latest evidence, we aim to close additional contracts which would eventually result in additional revenues when health care providers order the PreTRM test. We have built marketing capabilities, a national accounts team, and an inside sales team to sell and support the PreTRM test in key regions in the United States. Upon further market adoption of and more robust payment for the PreTRM test, and the expansion of our pipeline, we expect to expand our commercial team to more completely cover U.S. sales channels.
Intellectual Property
We rely on a combination of patents, trade secrets, copyrights and trademarks, as well as contractual protections, to establish and protect our intellectual property rights. Our success depends in part on our ability to obtain and maintain intellectual property protection for our tests and technology. In particular, we seek to protect the PreTRM test and any potential future products or services through a variety of methods, including seeking and maintaining patents intended to cover current and future products and services, their methods of use and processes for their manufacture, and any other inventions that are commercially important to the development of our business. We seek to obtain domestic and international patent protection which includes, in addition to filing and prosecuting patent applications in the United States, typically filing counterpart patent applications in additional countries where we believe such foreign filing is likely to be beneficial, including Europe, Japan, Canada, Australia and China.
As of December 31, 2023, our intellectual property portfolio encompasses three issued U.S. patents, five pending U.S. non-provisional patent applications, two international patent applications under the Patent Cooperation Treaty (PCT), 23 granted foreign patents in Canada, Poland, Switzerland, China, France, Germany, Italy, Ireland, Japan, Spain, Russia, Australia, Israel, the United Kingdom, and 17 member states of the European Union through a European patent with unitary effect, 26 pending foreign patent applications, and one U.S. provisional application. Our owned patents and patent applications, if issued, are expected to expire between 2034 and 2044, in each case without taking into account any possible patent term adjustments or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees.
Within our intellectual property portfolio, we own three patent families that relate to our PreTRM test. The patent applications of the first patent family include composition claims directed to panels of biomarkers and corresponding method claims for determining probability for preterm birth, gestational age at birth or time to birth in a pregnant female. The first patent family includes a pending U.S. patent application, eight foreign patents granted in Australia, China, France, Germany, Italy, Ireland, Spain, Canada, and the United Kingdom, and six pending foreign patent applications in the EPO, China, Australia, Japan, and Canada. The granted patents and pending patent applications, if issued, are expected to expire in 2034, without taking into account maintenance, renewal, annuity, or other governmental fees. The patent applications of the second patent family include composition claims directed to compositions of biomarkers, panels of biomarkers, and corresponding method claims for determining probability for preterm birth in a pregnant female, and discloses methods for determining probability of gestational diabetes. The second patent family includes two issued U.S. patents, 12 foreign patents granted in Japan, Russia, Australia, China, Israel, Ireland, Poland, Spain, Switzerland, the United Kingdom, and 17 member states of the European Union through a European patent with unitary effect, one pending U.S. patent application and eight pending foreign patent applications in the EPO, Canada, Australia, Japan, Hong Kong, Brazil, and China. The granted patents and pending patent applications, if issued, are expected to expire in 2036, without taking into account any possible patent term adjustment or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees. The patent application of the third patent family includes claims directed to antibodies and methods of using such antibodies for binding to specific biomarkers. The third patent family includes one international patent application under the PCT. The pending patent application, if issued, is expected to expire in 2043, without taking into account any possible patent term adjustment or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees.
We also own granted patents and pending patent applications directed to other indications. One patent family relates to determining probability for preeclampsia in a pregnant female, and includes two granted patents in Australia and Canada, and four patent applications pending in the U.S., the EPO, Australia and Canada. The granted patent and pending patent
applications, if issued, are expected to expire in 2034, without taking into account any possible patent term adjustment or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees. Similarly, another related patent family is directed to biomarker panels and methods for predicting preeclampsia in a pregnant female. This includes one international application under the PCT. Any granted patents from this application, if issued, are expected to expire in 2042, without taking into account any possible patent term adjustment or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees. A third patent family relates to determining probability for preterm birth associated with preterm premature rupture of membranes in a pregnant female. It includes patent applications pending in the U.S., the EPO, Canada, Japan, Australia, Israel, and China. The pending patent applications, if issued, are expected to expire in 2037, without taking into account any possible patent term adjustment or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees. A fourth patent family relates to determining the estimated due date for a pregnant female, and includes one granted patent in the U.S. and patent applications pending in the U.S., the EPO, Canada and Australia. The pending patent applications, if issued, are expected to expire in 2038, without taking into account any possible patent term adjustment or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees. A fifth patent family relates to pairs of biomarkers, compositions, and methods for predicting the probability for preterm birth in a pregnant female. It includes two pending applications in the U.S. and Canada. Any patent applications from this patent family, if issued, are expected to expire in 2042, without taking into account any possible patent term adjustment or extensions and assuming payment of all appropriate maintenance, renewal, annuity, or other governmental fees.
We also continue to file patent applications on new developments and improvements that may be important to our future business.
We cannot be sure that patents will be granted with respect to any of our pending patent applications or with respect to any patent applications we may own or license in the future, nor can we be sure that any of our existing patents or any patents we may own or license in the future will be useful in protecting our technology. Please see “Risk Factors — Risks Related to Our Intellectual Property” for additional information on the risks associated with our intellectual property strategy and portfolio.
We continually assess and refine our intellectual property strategy in order to fortify our position, and file additional patent applications when our intellectual property strategy warrants such filings. We intend to pursue additional intellectual property protection to the extent we believe it would be beneficial and cost-effective. Our ability to stop third parties from making, using, selling, offering to sell, importing or otherwise commercializing any of our patented inventions, either directly or indirectly, will depend in part on our success in obtaining, defending and enforcing patent claims that cover our technology, inventions, and improvements. With respect to our intellectual property, we cannot provide any assurance that any of our current or future patent applications will result in the issuance of patents in any particular jurisdiction, or that any of our current or future issued patents will effectively protect any of our tests or technology from infringement or prevent others from commercializing infringing tests or technology. Even if our pending patent applications are granted as issued patents, those patents may be challenged, circumvented or invalidated by third parties. Consequently, we may not obtain or maintain adequate patent protection for any of our tests or technology.
In addition to our reliance on patent protection for our inventions, tests and technology, we also rely on trade secrets, know-how, confidentiality agreements and continuing technological innovation to develop and maintain our competitive position. For example, some elements of manufacturing processes, analytics techniques and processes, as well as computational-biological algorithms, and related processes and software, are based on unpatented trade secrets and know-how that are not publicly disclosed. Although we take steps to protect our proprietary information and trade secrets, including through contractual means with our employees, advisors and consultants, these agreements may be breached and we may not have adequate remedies for any breach. In addition, third parties may independently develop substantially equivalent proprietary information and techniques or otherwise gain access to our trade secrets or disclose our technology. As a result, we may not be able to meaningfully protect our trade secrets. For further discussion of the risks relating to intellectual property, see the section titled “Risk factors — Risks Related to our Intellectual Property.”
Government Regulation
Federal and State Regulations Related to Clinical Laboratories
Clinical Laboratory Improvement Amendments of 1988
As a clinical laboratory, we are required to be certified under CLIA to conduct our business. Our clinical laboratory facility located in Salt Lake City, Utah holds a CLIA Certificate of Accreditation.
We are also accredited by CAP. CMS has deemed CAP standards to be equally or more stringent than CLIA regulations, and CAP is authorized to inspect the laboratories that it accredits on CMS’ behalf.
Under CLIA, a laboratory is any facility that performs laboratory testing on specimens derived from human beings for the purpose of providing information for the diagnosis, prevention, or treatment of disease or the impairment or assessment of health. CLIA requires that such laboratories obtain certification from the federal government and maintain compliance with various operational, personnel qualification, facilities administration, quality control and assurance, and proficiency testing requirements intended to ensure the accuracy, reliability, and timeliness of patient test results. CMS, part of the U.S. Department of Health and Human Services, or HHS, administers the CLIA certification program. CLIA certification is also necessary to bill state and federal health care programs, as well as many private insurers, for laboratory testing services.
CLIA requires that we hold a certificate that specifies the categories of testing we perform and that we comply with certain standards applicable to such tests. In addition, CLIA specifies certain testing categories requiring periodic proficiency testing, and certified laboratories performing these tests must enroll in an approved proficiency testing program.
In addition, as a condition of CLIA certification, our laboratory is subject to survey and inspection every other year, as well as random inspections. These biannual surveys are typically conducted by CAP because we hold a CLIA Certificate of Accreditation.
Laboratories like ours that perform high-complexity testing are required to meet more stringent requirements than laboratories performing less complex tests. A high-complexity CLIA-certified laboratory may develop, validate, and use proprietary tests referred to as laboratory developed tests, or LDTs. All of our current products are LDTs (as discussed further below under “Federal Oversight of Laboratory Developed Tests”). CLIA requires laboratories to demonstrate the analytical validity of any LDT used in clinical testing.
If our laboratory is determined to be out of compliance with CLIA requirements at any inspection or otherwise, we may be subject to sanctions such as suspension, limitation or revocation of our CLIA certificate, a directed plan of correction, on-site monitoring, civil monetary penalties, civil injunctive suits, criminal penalties, among other potential penalties, as well as significant adverse publicity, all of which may have a materially adverse impact on our business.
State Regulation of Clinical Laboratories
Our laboratory is located in Salt Lake City, Utah. Utah requires that laboratories located in this state hold a CLIA certificate (which we do), as well as approval by the Utah Department of Health, or UT DOH, to operate a laboratory. In addition to meeting CLIA requirements and holding a valid CLIA certificate, Utah requires that our laboratory timely notify the UT DOH of certain changes and demonstrate successful performance of proficiency testing in an approved proficiency testing program or approved alternative testing program. If our clinical laboratory is out of compliance with these standards, the UT DOH may revoke our approval to perform testing or potentially impose other remedial measures, any of which could materially affect our business. We maintain an approval in good standing with the UT DOH.
CLIA provides that a state may adopt laboratory regulations that are more stringent than those under federal law, and one such state, New York, has implemented its own more stringent laboratory regulatory requirements. Additionally, several states require the licensure of out-of-state laboratories that accept specimens from those states and/or receive specimens from laboratories in those states. One such state is New York. We have obtained licenses from states where we believe we are required to be licensed. Other states beyond those from which our laboratory currently holds licenses may adopt licensure requirements in the future, which could require us to modify, delay, or discontinue our operations in such jurisdictions. If we identify any other state with such requirements or if we are contacted by any other state advising us of such requirements, we intend to follow instructions from the state regulators as to how to comply with such requirements.
In addition, as part of the laboratory licensure process, the New York State Department of Health, or NY DOH, requires that laboratories seeking licensure establish the analytic and clinical performance characteristics of all tests performed, and also imposes specific review and approval requirements on certain categories of testing, including LDTs. As an LDT, our PreTRM test is subject to this NY DOH review and approval process.
If a laboratory is out of compliance with state laws or regulations governing licensed laboratories, penalties may include suspension, limitation or revocation of the license, assessment of financial penalties or fines, or imprisonment. Loss of a laboratory’s state license may also result in the inability to receive payments from state and federal health care programs as well as private insurers, all of which may have a materially adverse impact on our business.
Regulation of Clinical Trials
We have conducted and are currently conducting a variety of studies for the PreTRM test and our other tests in development that involve clinical investigators at multiple sites in the U.S. We may need to conduct additional studies for the PreTRM test, as well as other tests we may offer in the future, to drive test adoption in the marketplace and reimbursement. Should we not be able to perform these studies, or should their results not provide clinically meaningful data and value for clinicians, adoption of our tests could be impaired and we may not be able to obtain reimbursement for them.
The conduct of clinical trials is also subject to extensive federal and institutional regulations, which regulations are intended to assure that the data and reported results are credible and accurate, and that the rights, safety, and welfare of study participants are protected. Most studies involving human participants must be reviewed and approved by, and conducted under the auspices of, a duly-constituted institutional review board, or IRB, which is a multi-disciplinary committee responsible for reviewing and evaluating the risks and benefits of a clinical trial for participating subjects and monitoring the trial on an ongoing basis. Companies sponsoring the clinical trials and investigators also must comply with, as applicable, regulations, guidelines and IRB requirements for obtaining informed consent from the study subjects, following the protocol and investigational plan, adequately monitoring the clinical trial, and timely reporting of adverse events. We believe our clinical trials conducted to date have met applicable regulatory requirements. The sponsoring company or the IRB may suspend or terminate a clinical trial at any time on various grounds, including a finding that the subjects are being exposed to an unacceptable health risk. In addition, studies involving human participants often require significant time and cash resources to complete and are subject to a high degree of risk, including risks of experiencing delays, failing to complete the trial or obtaining unexpected or negative results.
The International Committee of Medical Journal Editors, or ICMJE, requires trial registration as a condition of the publication of research results generated by a clinical trial. To fulfill this obligation organizations and individuals can provide the information required by ICMJE either to ClinicalTrials.gov, which is maintained by the U.S. National Institutes of Health, or to a World Health Organization registry. In accordance with this publication policy to ensure that our investigators can publish their findings, and to further our participant enrollment activities for various studies, we register all of the clinical trials that we sponsor with ClinicalTrials.gov.
Federal Oversight of Laboratory Developed Tests
Our first commercial product, the PreTRM test, is an LDT that we process in our single CLIA-certified central laboratory. Although the Food and Drug Administration, or FDA, has asserted that it has authority to regulate LDTs, it has historically exercised enforcement discretion to regulate most tests developed, manufactured and performed within a single high-complexity CLIA-certified laboratory. In October 2023, FDA issued a proposed rule aimed at regulating LDTs under the current medical device framework. The agency’s proposal also includes a plan to phase out its current enforcement discretion policy over several years, as discussed further below. Any changes in FDA’s approach to regulation of LDTs generally, or its approach to regulating the PreTRM test specifically, could adversely impact our business.
FDA Oversight of LDTs
While clinical laboratory tests are regulated under CLIA, which is administered by CMS, as well as by applicable state laws, the FDA separately has jurisdiction over medical devices pursuant to its authority under the Food, Drug, and Cosmetic Act, or FD&C Act. In vitro diagnostic devices, or IVDs, intended for clinical purposes are a type of medical device under the FD&C Act and thus fall within the FDA’s jurisdiction, and the agency applies its authority under the FD&C Act to those IVDs and test kits that are manufactured, packaged, and distributed in interstate commerce. LDTs are considered to be a subset of IVDs that are designed, manufactured, and used within a single laboratory. The FDA regulates,
among other matters, the research, testing, manufacturing, safety, labeling, storage, recordkeeping, premarket clearance or approval, marketing and promotion and sales and distribution of medical devices, including IVDs, in the U.S. to ensure that such products on the domestic market are safe and effective for their intended uses. In addition, the FDA regulates the import and export of medical devices. Many of the instruments, reagents, kits or other consumable products used within our laboratory are regulated as medical devices and therefore must comply with FDA quality system regulations and certain other device requirements. We have policies and procedures in place to ensure that we source such materials from suppliers that are in compliance with any applicable medical device regulatory requirements.
Although the FDA has statutory authority to ensure that medical devices, including IVDs, are safe and effective for their intended uses, the FDA historically exercised enforcement discretion and generally did not enforce applicable provisions of the FD&C Act and regulations with respect to LDTs. Despite its exercise of enforcement discretion, there have been numerous proposals over the years to modify how LDTs may be brought into a harmonized paradigm for oversight by the FDA and CMS. As noted above, the FDA issued a proposed rule in October 2023 that is intended to regulate LDTs under the current medical device framework and to phase out the agency’s existing enforcement discretion policy for this category of diagnostic tests. The public comment period for this proposed rule ended in early December 2023. The proposal envisions that the LDT enforcement policy phase-out process would occur in gradual stages over a total period of four years, with premarket approval applications for high-risk tests to be submitted by the 3.5-year mark, although more details are expected to be provided with the upcoming final rule. The likelihood of the FDA finalizing the proposed rule in April 2024 (as currently projected), as well as potential litigation challenging the agency’s authority to take such action, is uncertain at this time. Affected stakeholders continue to press for a comprehensive legislative solution to create a harmonized paradigm for oversight of LDTs by both the FDA and CMS, instead of implementation of the proposed FDA administrative action, which may be disruptive to the industry and to patient access to certain diagnostic tests.
Separately, federal legislators have been working with stakeholders for several years on a possible bill to reform the regulation of in vitro diagnostic tests, including LDTs. For example, as drafted and re-introduced for consideration by the current Congress, reform legislation called the Verifying Accurate, Leading-edge IVCT Development, or VALID, Act would codify the term “in vitro clinical test”, or IVCT, and create a new medical product category separate from medical devices that includes products currently regulated as IVDs as well as LDTs, among other provisions. The VALID Act would also create a new system for laboratories to use to submit their tests electronically to the FDA for approval, which is aimed at reducing the amount of time it would take for the agency to approve such tests, and establish a new program to expedite the development of diagnostic tests that can be used to address a current unmet need for patients.
If Congress were to pass the VALID Act or any other legislation applicable to the FDA’s regulation of LDTs, or if the FDA finalizes its LDT proposed rule through the ongoing notice-and-comment rulemaking process, we will likely become subject to increased regulatory burdens such as registration and listing requirements, adverse event reporting requirements, and quality control requirements. Any legislation or formal FDA regulatory framework affecting LDTs is also likely to have premarket application requirements prohibiting commercialization without FDA authorization and controls regarding modification to the tests that may require further FDA submissions. Any such process would likely be costly and time-consuming, and we cannot assure that the PreTRM test, or any new tests that we may develop, will be authorized for marketing by the FDA in a timely or cost-effective manner, if at all.
Moreover, if the FDA were to disagree with our conclusion that the PreTRM test falls within the scope of the agency’s existing LDT definition and enforcement discretion policies, and the agency thus asserts that the PreTRM test is subject to FDA’s medical device authorities and implementing regulations, the agency could require that we obtain premarket approval or another type of device premarket authorization in order for us to commercialize the PreTRM test. As part of this process, we may also be required to conduct additional clinical testing before applying for commercial marketing authorization. Clinical trials must be conducted in compliance with FDA regulations in order to support a marketing submission to the agency for a regulated product, or the FDA may take certain enforcement actions or reject the data. Performing additional, new clinical studies and trials in order to obtain product approval from the FDA, if necessary, would take a significant amount of time and would substantially delay our ability to commercialize the PreTRM test, all of which would adversely impact our business. In addition, the Consolidated Appropriations Act for 2023 recently amended the FD&C Act to require sponsors of most clinical studies of investigational medical devices intended to support marketing authorization to develop and submit a diversity action plan for such clinical trial. The action plan must include the sponsor’s diversity goals for enrollment, as well as a rationale for the goals and a description of how the sponsor will meet them. It is unknown at this time how the diversity action plan may affect the planning and timing of medical device investigations or what specific information the FDA will expect in such plans, but if the FDA objects to a sponsor’s diversity action plan, it may delay trial initiation or review of the device’s premarket submission.
Advertising of Laboratory Services and LDTs
Our advertising for laboratory services and tests is subject to federal truth-in-advertising laws enforced by the Federal Trade Commission, or FTC, as well as certain state laws.
Under the Federal Trade Commission Act, or FTC Act, the FTC is empowered, among other things, to (i) prevent unfair methods of competition and unfair or deceptive acts or practices in or affecting commerce; (ii) seek monetary penalties and other relief for conduct injurious to consumers; and (iii) gather and compile information and conduct investigations relating to the organization, business, practices, and management of entities engaged in commerce. The FTC has very broad enforcement authority, and failure to abide by the substantive requirements of the FTC Act and other consumer protection laws can result in administrative or judicial penalties, including civil penalties, injunctions affecting the manner in which we would be able to market services or products in the future, or criminal prosecution. In recent years, the FTC has become more active in its scrutiny of health claims used in advertising goods and services, including with its publications of a sweeping “health products compliance guidance” document in December 2022.
Data Privacy and Security Laws
We believe that we have taken the steps required of us to comply with both federal and state health information privacy and security statutes and regulations, including genetic testing and genetic information privacy laws. However, existing laws regulating such matters continue to evolve, including through amendments, new interpretations and guidance, and, around the world, lawmakers continue to propose new laws regulating privacy and data security. We may not be able to maintain compliance in all jurisdictions where we do business. Failure to maintain compliance, or changes in laws regarding privacy or security could result in civil and/or criminal penalties, significant reputational damage and could have a material adverse effect on our business.
Federal Privacy and Security Laws
The Health Insurance Portability and Accountability Act of 1996, or HIPAA, established comprehensive federal standards for the privacy and security of health information. The HIPAA standards apply to health plans, health care clearing houses, and health care providers that conduct certain health care transactions electronically (Covered Entities), as well as their respective business associates that perform services for them that involve the use, or disclosure of, individually identifiable health information. Title II of HIPAA, the Administrative Simplification Act, contains provisions that address the privacy and security of health data, the standardization of identifying numbers used in the health care system and the standardization of certain health care transactions. The privacy regulations protect medical records and other protected health information by limiting their use and release, giving patients the right to access their medical records and limiting most disclosures of health information to the minimum amount necessary to accomplish an intended purpose. The HIPAA security standards require the adoption of administrative, physical, and technical safeguards and the adoption of written security policies and procedures.
In 2009, Congress enacted Subtitle D of the Health Information Technology for Economic and Clinical Health Act. or HITECH provisions of the American Recovery and Reinvestment Act of 2009. HITECH amended HIPAA and, among other things, expanded and strengthened HIPAA, created new targets for enforcement, imposed new penalties for noncompliance and established new breach notification requirements for Covered Entities and Business Associates. Regulations implementing major provisions of HITECH were finalized on January 25, 2013 through publication of the HIPAA Omnibus Rule. The Omnibus Rule contained significant changes for Covered Entities and Business Associates with respect to compliance obligations and dramatically increased penalties for noncompliance.
Under HITECH’s breach notification requirements, Covered Entities must report breaches of protected health information that has not been encrypted or otherwise secured in accordance with guidance from the Secretary of HHS, or the Secretary. Required breach notices must be made as soon as is reasonably practicable, but no later than 60 days following discovery of the breach. Reports must be made to affected individuals and to the Secretary and, in some cases depending on the size of the breach and location of affected individuals, they must be reported through local and national media. Breach reports can lead to investigation, enforcement and civil litigation, including class action lawsuits. We are currently subject to the HIPAA regulations as a Covered Entity and maintain an active compliance program. We are subject to audit by HHS as well as compliance reviews. We may also be investigated in connection with a privacy or data security complaint.
There are significant civil and criminal fines and other penalties that may be imposed for violating HIPAA. These fines are adjusted for inflation each year. A Covered Entity or business associate is liable for civil monetary penalties for a violation that is based on an act or omission of any of its agents, including a downstream business associate, as determined according to the federal common law of agency. Penalties for failure to comply with a requirement of HIPAA and HITECH vary significantly depending on the nature of the failure and include civil monetary penalties. A single breach incident can violate multiple requirements.
Additionally, a person who knowingly obtains or discloses protected health information in violation of HIPAA may face a criminal penalties, which increase if the wrongful conduct involves false pretenses or the intent to sell, transfer or use information for commercial advantage, personal gain or malicious harm. Proposed modifications to the HIPAA Privacy Rule were published in January of 2021 with a public comment period that ended in May of 2021. Final rules have not yet been published by HHS, therefore, the content of any final rules and their impact on us is not yet known.
Further, submission of electronic health care claims and payment transactions that do not comply with the electronic data transmission standards established under HIPAA and HITECH could result in delayed or denied payments. Any non-compliance with HIPAA and HITECH, and related penalties, could adversely impact our business.
State Privacy and Security Laws
In addition to federal enforcement, Covered Entities are also subject to enforcement by state attorneys general who were given authority to enforce HIPAA under HITECH. HIPAA privacy, security, and breach notification regulations do not supersede state laws that are more stringent or provide individuals with greater privacy and security rights or greater access to their records and we are subject to enforcement by state regulatory authorities for failure to comply with more stringent state laws.
The compliance requirements of these laws, including additional breach reporting requirements, and the penalties for violation vary widely and new privacy and security laws in this area are evolving. For example, several states, such as California, have implemented comprehensive privacy laws and regulations. The California Confidentiality of Medical Information Act imposes restrictive requirements regulating the use and disclosure of individually identifiable health information. In addition to fines and penalties imposed upon violators, some of these state laws also afford private rights of action to residents who believe their personal information has been misused.
California has also adopted the California Consumer Privacy Act of 2018, or CCPA, which took effect on January 1, 2020 and became enforceable by the state attorney general on July 1, 2020. The CCPA establishes a new privacy framework for covered businesses by creating an expanded definition of personal information, establishing new data privacy rights for consumers in the State of California, imposing special rules on the collection of consumer data from minors, and creating a new and potentially severe statutory damages framework for violations of the CCPA and for businesses that fail to implement reasonable security procedures and practices to prevent data breaches.
The regulations issued under the CCPA have been modified several times. Additionally, the California Privacy Rights Act, or CPRA, was approved by California voters on November 3, 2020 and went into effect in January 2023 modifying the CCPA significantly, resulting in further uncertainty, additional costs and expenses stemming from efforts to comply, and additional potential for harm and liability for failure to comply. CPRA established a new regulatory authority, the California Privacy Protection Agency (CPPA) responsible for enacting and enforcing new regulations under its expanded enforcement authority. CPRA required the CPPA to finalize regulations by July 1, 2022 but the agency did not complete the first batch of rules until March 29, 2023. Immediately following publication of the rules, the California Chamber of Commerce, or CCC, filed suit challenging the enforcement date of the new rules, scheduled for July 1, 2023 or one-year following publication of the rules, arguing that the statutory intent was for the regulated entities to have a full year to comply with new requirements and arguing for an effective date of March 29, 2024. A state district court agreed with the CCC but the district court’s decision to delay enforcement was reversed on appeal permitting immediate enforcement by CPPA. CPPA has publicly warned regulated entities to prepare for immediate enforcement action. Other states in the U.S. have implemented privacy laws similar to the CCPA. In February 2021, Virginia and Colorado enacted similar data protection laws and since then, a number of other U.S. states have enacted similar proposals, increasing the regulatory compliance risk. In dealing with health information for the development of our technology or for commercial purposes, we will be indirectly affected by HIPAA and state-imposed health information privacy and security laws because these laws regulate the ability of our potential customers and research collaborators to share health information with us. Additionally, we must identify and comply with all applicable state laws for the protection of personal information with respect to employee information or other personal information that we collect.
Other Federal and State Health Care Laws
A variety of state and federal laws prohibit fraud and abuse involving private insurers (as well as state and federal health care programs). These laws are interpreted broadly and enforced aggressively by various state and federal agencies, including CMS, the Department of Justice, or DOJ, the Office of Inspector General for the Department of Health and Human Services, or OIG, and various state agencies. Sanctions for violations of these laws may result in a range of penalties, including but not limited to significant criminal and civil fines and penalties, and loss of licensure. Any such penalties would adversely affect our business.
Anti-Kickback Statute
The Anti-Kickback Statute, or AKS, prohibits, among other things, knowingly and willfully offering, paying, soliciting, or receiving remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual, or the furnishing, arranging for or recommending of an item or service that is reimbursable, in whole or in part, by a federal health care program. “Remuneration” is broadly defined to include anything of value, which can include (but is not limited to) cash payments, gifts or gift certificates, discounts, or the furnishing of services, supplies or equipment. A person or entity does not need to have actual knowledge of the federal AKS or specific intent to have committed a violation. In addition, a claim including items or services resulting from a violation of the AKS constitutes a false or fraudulent claim for purposes of the federal False Claims Act, or FCA.
The AKS has safe harbors and exceptions that protect certain conduct and arrangements that meet every element of the applicable safe harbor or exception. However, an arrangement that does not meet all elements of a safe harbor or exception does not necessarily violate the AKS. A facts-and-circumstances analysis of the arrangement or conduct at issue is necessary to determine whether a potential violation has occurred. Some states have their own AKS provisions, including statutes that apply to claims submitted to private insurers. Some of these statutes have their own safe harbor provisions or exceptions, or they may cross-reference the AKS safe harbors.
The penalties for violating federal or state AKS provisions can be severe. Possible sanctions include criminal and civil penalties (including penalties under the FCA or a state law equivalent), imprisonment, and possible exclusion from state or federal health care programs.
From time to time, the OIG has issued Special Fraud Alerts describing the agency’s view of how certain arrangements between laboratories and referring physicians implicate and potentially violate the AKS. For example, the OIG issued such Alerts in December 1994 and June 2014, and an Alert related to speaker programs issued in November 2020 also applies to the business of laboratories. These Special Fraud Alerts do not have the force of law, but do provide insight into the agency’s potential enforcement priorities and its interpretation of the AKS as it relates to laboratories’ business practices. Similarly, state enforcement agencies may issue opinion letters or other guidance documents that describe their interpretation of how the state AKS applies to certain arrangements, and also provide insight into that agency’s enforcement priorities.
Physician Self-Referral Prohibitions
Subject to certain exceptions, the federal ban on physician self-referrals (referred to as the Stark Law) is a civil statute that prohibits physicians from referring Medicare and Medicaid patients to an entity providing certain designated health services, which include laboratory services, if the physician or his/her immediate family member has any financial relationship with the entity. Many states also have their own self-referral bans, which may extend to all self-referrals regardless of the payer, unless an exception applies.
Potential penalties for Stark Law violations include the return of funds received for all prohibited referrals, fines, civil monetary penalties (including penalties under the FCA or state law equivalents), and possible exclusion from state or federal health care programs.
Eliminating Kickbacks in Recovery Act
In October 2018, Congress enacted the Eliminating Kickbacks in Recovery Act of 2018, or EKRA, as part of the Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act, or SUPPORT Act. EKRA is an all-payer anti-kickback law that criminalizes paying any remuneration to induce referrals to, or in exchange for, patients using the services of a recovery home, a substance use clinical treatment facility, or laboratory.
Although it appears that EKRA was intended to reach patient brokering and similar arrangements in the context of substance use recovery and treatment, EKRA’s language is broad. For example, as written, EKRA seems to prohibit the payment of incentive compensation to sales employees, whereas such payments are expressly protected under the AKS and its safe harbors (and this practice is common in the industry). And most of the safe harbors available under the AKS are not reiterated under EKRA’s exceptions. Therefore, compliance with an AKS safe harbor may not guarantee protection under EKRA. EKRA thus potentially expands the universe of arrangements that could be subject to enforcement under federal fraud and abuse laws, as well as substantial penalties.
EKRA permits DOJ to issue regulations clarifying or expanding the statute’s exceptions, but such regulations have not yet been issued. Because, moreover, EKRA is a new law, there is little guidance to indicate how and to what extent it will be applied and enforced by government agencies. The relationships between laboratories and physicians, sales representatives, hospitals, and customers may be subject to scrutiny under this statute. If imposed for any reason, sanctions under EKRA could have a negative effect on our business.
False Claims Act
The FCA imposes civil liability on any person or entity that, among other things, knowingly presents, or causes to be presented, to the federal government, claims for payment that are false or fraudulent; knowingly making, using or causing to be made or used, a false statement or record material to a false or fraudulent claim or obligation to pay or transmit money or property to the federal government or knowingly concealing or knowingly and improperly avoiding or decreasing an obligation to pay money to the federal government. The FCA also prohibits the knowing retention of overpayments (sometimes referred to as “reverse false claims”). Under the reverse false claims provision, improperly retained overpayments must be repaid within 60 days of identification unless a favorable decision is obtained on appeal. The FCA also permits a private individual acting as a “whistleblower” (also referred to as a qui tam relator) to bring actions on behalf of the federal government alleging violations of the FCA and to share in any monetary recovery. The federal government may elect or decline to intervene in such matters, but if the government declines intervention, the whistleblower may still proceed with the litigation on the government’s behalf.
Penalties for violating the FCA include payment of up to three times the actual damages sustained by the government, plus substantial per-claim civil penalties, as well as possible exclusion from federal health care programs.
Various states have enacted similar laws modeled after the FCA that apply to items and services reimbursed under Medicaid and other state health care programs, and, in several states, such laws apply to claims submitted to any payer, including private insurers.
There is also a federal criminal false claims statute that prohibits, in pertinent part, the making or presentation of a false claim, knowing such claim to be false, to any person or officer in the civil, military, or naval service or any department or agency thereof.
Health Care Fraud and False Statements
The federal health care fraud statute criminalizes knowingly and willfully defrauding a health care benefit program, including private insurers. A violation of this statute may result in fines, imprisonment, or exclusion from government health care programs. The false statements statute prohibits knowingly and willfully falsifying, concealing, or covering up a material fact or making a materially false, fictitious, or fraudulent statement in connection with the delivery of or payment for health care benefits, items, or services. A violation of this statute may result in fines or imprisonment.
Civil Monetary Penalties Law
The federal Civil Monetary Penalties Law, or CMP Law, prohibits, among other things, (1) the offering or transfer of remuneration to a Medicare or Medicaid beneficiary if the person knows or should know that remuneration is likely to influence the beneficiary’s selection of a particular provider, practitioner, or supplier of services reimbursable by Medicare or a state health care program, unless an exception applies; (2) employing or contracting with an individual or entity that the provider knows or should know is excluded from participation in a federal health care program; (3) billing for services requested by an unlicensed physician or an excluded provider; and (4) billing for medically unnecessary services. The penalties for violating the CMP Law include exclusion from participation in federal health care programs, substantial fines, and payment of up to three times the amount billed, depending on the nature of the offense.
Physician Payments Sunshine Act
In pertinent part, the federal Physician Payments Sunshine Act, or Sunshine Act, imposes reporting requirements on manufacturers of certain devices, drugs and biologics reimbursed under Medicare, Medicaid, or the Children’s Health Insurance Program, or CHIP, for certain payments and transfers of value by them (and in some cases their distributors) to physicians, teaching hospitals and certain advanced non-physician health care practitioners, as well as ownership and investment interests held by physicians and their immediate family members. The reporting program (known as the Open Payments program) is administered by CMS. A number of states also have laws similar to the Sunshine Act.
Because we develop our LDTs solely for use by or within our own laboratory, we believe we are exempt from these reporting requirements. We could, however, become subject to such reporting requirements under the terms of current CMS regulations if the FDA finalizes its recently initiated notice-and-comment rulemaking to exercise authority over LDTs as medical devices or otherwise requires us to obtain premarket clearance or approval for our tests as medical devices or Congress enacts legislative reforms to the federal oversight of LDTs to subject them to FDA regulation and/or the reporting requirements of the Sunshine Act.
Other Potentially Applicable State Laws
We are subject to state and foreign equivalents of each of the health care laws and regulations described above, among others, some of which may be broader in scope and may apply regardless of the payer. Many U.S. states have adopted laws similar to the AKS and FCA, and may apply to our business practices, including, but not limited to, research, distribution, sales or marketing arrangements and claims involving health care items or services reimbursed by non-governmental payers, including private insurers. Such laws include fee-splitting restrictions, insurance fraud laws, anti-markup laws, prohibitions on waiving coinsurance, copayments, deductibles and other amounts owed by patients, and prohibitions on the provision of tests at no or discounted cost to induce physician adoption. Other potentially applicable state laws include direct billing requirements and prohibitions on the corporate practice of medicine. Many of our agreements may be subject to such laws. There are ambiguities as to what is required to comply with these state requirements, and if we fail to comply with an applicable state law requirement we could be subject to penalties. Finally, there are state laws governing the privacy and security of health information, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
Reimbursement and Billing
Coverage and Reimbursement
In the United States and markets in some other countries, patients generally rely on third-party payers to reimburse all or part of the costs associated with their treatment. Adequate coverage and reimbursement from government health care programs, such as Medicare and Medicaid, and commercial insurers is critical to new product acceptance. Our ability to successfully commercialize our products will depend in part on the extent to which coverage and adequate reimbursement for these products and related treatments will be available from government health care programs, commercial insurers and other third-party payers. Third-party payers, including managed care organizations (“MCOs”) and other commercial insurers, decide which medical products and services they will pay for and establish reimbursement levels. The availability of coverage and extent of reimbursement by third-party payers is essential for most patients to be able to afford treatments. Sales of the PreTRM test or other clinical testing that we may develop will in large part depend, both domestically and abroad, on the extent to which the costs of our tests will be paid by MCOs or other commercial insurers, or reimbursed by government health care programs, and other third-party payers. If coverage and adequate reimbursement is not available, or is only partially available, we may not be able to successfully continue to commercialize our tests. Even if coverage is provided, the approved reimbursement amount may not be high enough to allow us to establish or maintain pricing sufficient to realize a sufficient return on our investment.
Factors payers consider in determining reimbursement are based on whether the product is:
•a covered benefit under its health plan;
•safe, effective and medically necessary;
•appropriate for the specific patient;
•cost-effective; and
•neither experimental nor investigational.
In addition, market-based changes have affected and will continue to affect the clinical laboratory business. Reimbursement from private insurers for diagnostic testing may shift away from traditional, fee-for-service models to alternatives, including value-based, bundled, and other risk-sharing payment models.
The growth of the managed care sector and consolidation of MCOs may also present various challenges and opportunities to us and other clinical laboratories. For example, MCOs have different contracting philosophies. Some MCOs contract with a limited number of clinical laboratories and engage in direct negotiation of rates, while others adopt broader networks with more uniform fee structures for participating clinical laboratories, and still others use capitation rates to fix the cost of laboratory testing services for enrollees. Our revenues may vary depending on the MCOs with which we enter contracts, if we decide to enter such contracts.
In addition to the potential reductions in test reimbursement, we may also see a decline or change in test volumes as a result of increased controls over the utilization of laboratory services by third-party payers, particularly MCOs. For example, MCOs have implemented, either directly or through third parties, various types of laboratory benefit management programs, which may include lab networks, utilization management tools (such as prior authorization and/or prior notification), and claims edits, which impact coverage and reimbursement of clinical laboratory tests. Some of these programs address clinical laboratory testing broadly, while others are focused on certain types of testing.
Despite the potentially negative market changes related to reimbursement, several factors may positively impact test volume, including the expansion of managed care and private insurance exchanges. In addition, continued innovation in laboratory medicine may continue to foster greater appreciation of the value of women’s health diagnostics. Additional factors that may lead to future volume growth include an increase in the number and types of tests that are readily available (due to advances in technology and increased cost efficiencies).
The Protecting Access to Medicare Act of 2014
Reimbursement and billing for diagnostic services is highly complex. Laboratories must bill various payers, including private insurers and MCOs. Submitting claims to various payers is complicated because each payer may have different billing requirements. Additionally, the audit requirements laboratories must meet to ensure compliance with applicable laws and regulations, as well as internal compliance policies and procedures, add further complexity to the billing process.
In April 2014, Congress passed the Protecting Access to Medicare Act of 2014, or PAMA, which substantially changed the way in which clinical laboratory services are paid under Medicare’s Clinical Laboratory Fee Schedule, or CLFS.
PAMA took effect on January 1, 2018 and requires certain clinical laboratories to report to CMS private insurer payment rates and volumes for their tests, though the reporting requirement has been delayed. CMS then takes the weighted-median of payments made by private insurers for these tests to set reimbursement under the CLFS for qualifying tests, subject to certain phase-in limits. Laboratories that fail to report the required payment information may be subject to substantial civil monetary penalties.
Since December 2019, Congress has passed a series of laws to modify PAMA’s statutory requirements related to the data reporting period and phase-in of payment reductions under the CLFS for clinical diagnostic laboratory tests, or CDLTs, that are not advanced diagnostic laboratory tests, or ADLTs. Most recently, the Further Continuing Appropriations and Other Extensions Act of 2024 (Pub.L. 118-22, enacted on November 16, 2023) further delayed the reporting requirement as well as the application of the 15% phase-in reduction. Under these statutory provisions, the next data reporting period for CDLTs that are not ADLTs will be January 1, 2025 through March 31, 2025, and will be based on the most recent data collection period of January 1, 2019 through June 30, 2019. After this data reporting period, the three-year data reporting cycle for these tests will resume (e.g., 2028, 2031, etc.).
The same series of laws modified the phase-in of payment reductions resulting from private payer rate implementation so that a 0.0% reduction limit was applied for calendar years, or CYs, 2021 through 2023, as compared to the payment amounts for a test the preceding year. The Further Continuing Appropriations and Other Extensions Act of 2024 further
applied a 0.0% reduction limit for CY 2024. Consequently, payment may not be reduced by more than 15% per year for CYs 2025 through 2027 as compared to the payment amounts established for a test the prior year.
CMS’s methodology under PAMA (as well as the willingness of private insurers to recognize the value of diagnostic testing and pay for that testing accordingly) renders private insurer payment levels even more significant. This calculation methodology has resulted in significant reductions in reimbursement, even though CMS imposed caps on those reductions. The reduction of reimbursement under the CLFS also affects rates paid by private insurers because those insurers often set their pricing for laboratory testing as a percentage of the amount set on the CLFS.
Following the implementation of a unique PLA code for the PreTRM test in April 2021, CMS priced this code at $750 under the PAMA framework in November 2021. While this price and how it may change over time under PAMA directly affect Medicare reimbursement for our testing, we do not currently bill Medicare in any material amount for our tests. However, PAMA and the price set by CMS have an indirect effect on rates paid by commercial insurers.
Given the many uncertainties built into PAMA’s price-setting process, we cannot predict how payments we receive from private insurers (or possibly from Medicare in the future), and thus our revenue, may change from year to year.
Health Care Reform and Legislation
We likewise cannot predict whether or when Congress or state legislatures may take steps to regulate or change pricing of laboratory testing, and thus affect the reimbursement we receive as well as our revenue. Examples of such initiatives might include changes to the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010, or collectively the ACA, steps to address surprise billing, and increased price transparency, as well as administrative requirements that may continue to affect coverage, reimbursement, and utilization of laboratory services in ways that are currently unpredictable.
Since its enactment, there have been multiple attempts to repeal the ACA or significantly scale back its applicability, as a result of which, certain sections of the ACA have not been fully implemented or were effectively repealed. This could negatively impact reimbursement for our testing, adversely affect our test volumes and adversely affect our business, operating results, and financial condition. However, following several years of litigation in the federal courts, in June 2021, the United States Supreme Court upheld the ACA when it dismissed a legal challenge to the Act’s constitutionality. Further legislative and regulatory changes to federal health care laws and policies remain possible. Future changes or additions to the ACA, the Medicare and Medicaid programs, and changes stemming from other health care reform measures, especially with regard to health care access, financing or other legislation in individual states, could have a material adverse effect on the health care industry in the U.S. For example, in August 2022 President Biden signed into law the Inflation Reduction Act, which provides CMS with new authorities to negotiate drug prices annually for certain prescription drug products covered by Medicare starting for plan year 2026. This recent development signals a potential shift in the willingness of federal policy makers to more aggressively regulate the pricing of medical goods and services that are offered for sale in the U.S. The uncertainty around the future of the ACA and other health care legislation, and in particular the impact to reimbursement levels and the number of insured individuals, may lead to delay in the purchasing decisions of our customers.
Other legislative changes have been proposed and adopted in the United States since the ACA was enacted. For example, the Budget Control Act of 2011, among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several state and federal health care programs. This includes aggregate reductions of Medicare payments to providers up to 2% per fiscal year, and, due to subsequent legislative amendments, will remain in effect through 2032 unless additional Congressional action is taken (with the exception of a temporary suspension from May 1, 2020 through March 31, 2022 due to the COVID-19 pandemic). As another example, in January 2013, the American Taxpayer Relief Act of 2012 was signed into law, which, among other things, increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
Other Applicable Environmental, Health, And Safety Regulations
We are subject to numerous federal, state and local environmental, health and safety, or EHS, laws and regulations relating to, among other matters, safe working conditions, environmental protection, and handling or disposition of
products, including those governing the generation, storage, handling, use, transportation, release, and disposal of hazardous or potentially hazardous materials, medical waste, and infectious materials.
Some of these laws and regulations also require us to obtain licenses or permits to conduct our operations. If we fail to comply with such laws or obtain and comply with the applicable permits, we could face substantial fines or possible revocation of our permits or limitations on our ability to conduct our operations.
Certain of our development activities involve use of hazardous materials, and we believe we are in compliance with the applicable environmental laws, regulations, permits, and licenses. However, we cannot ensure that EHS liabilities will not develop in the future. EHS laws and regulations are complex, change frequently and have tended to become more stringent over time.
Although the costs to comply with applicable laws and regulations, we cannot predict the impact on our business of new or amended laws or regulations or any changes in the way existing and future laws and regulations are interpreted or enforced, nor can we ensure we will be able to obtain or maintain any required licenses or permits.
Human Capital
As of December 31, 2023, we had 57 employees, including 55 full-time employees. Our headquarters are located in Salt Lake City, Utah. None of our employees are subject to a collective bargaining agreement. We consider our relationship with our employees to be good.
Talent Acquisition and Retention
We recognize that our employees largely contribute to our success. To this end, we support business growth by seeking to attract and retain best-in-class talent. We use internal and external resources to recruit highly skilled candidates for open positions. We believe that we are able to attract and retain superior talent as measured by our low turnover rate and high employee service tenure.
Total Rewards
Our total rewards philosophy has been to create investment in our workforce by offering a competitive compensation and benefits package. We provide employees with compensation packages that include base salary, annual incentive bonuses and long-term equity incentive awards. We also offer comprehensive employee benefits, such as life, disability and health insurance, health savings and flexible spending accounts, paid time off, and a 401(k) plan. It is our express intent to be an employer of choice in our industry by providing a market-competitive compensation and benefits package.
Health, Safety and Wellness
We have always invested, and will continue to invest, in the health, safety, and wellness of our employees. We provide our employees with access to a variety of innovative, flexible, and convenient health and wellness programs. Program benefits are intended to provide protection and security, so employees can have peace of mind concerning events that may require time away from work or that may impact their financial well-being.
Diversity, Equity, and Inclusion
We believe a diverse workforce is critical to our success. Our mission is to value differences in races, ethnicities, religions, nationalities, genders, ages and sexual orientations, as well as education, skill sets and experience. We are focused on inclusive hiring practices, fair and equitable treatment, organizational flexibility and training and resources.
Training and Development
We believe in encouraging employees in becoming lifelong learners by providing ongoing learning and leadership training opportunities. While we strive to provide real-time recognition of employee performance, we have a formal annual review process not only to determine pay and equity adjustments tied to individual contributions, but to identify areas where training and development may be needed.
Information About Our Executive Officers and Directors
The following persons were our executive officers and directors as of March 15, 2024:
| | | | | | | | |
| Name | | Position |
| Executive Officers | | |
| Zhenya Lindgardt | | President and Chief Executive Officer |
| Austin Aerts | | Chief Financial Officer |
| John J. Boniface, Ph.D. | | Chief Scientific Officer |
| Paul Kearney, Ph.D. | | Chief Data Officer |
| Robert G. Harrison | | Chief Information Officer |
| Benjamin G. Jackson | | General Counsel |
| Directors | | |
| Jane F. Barlow, M.D. | | Chief Executive Officer, Jane Barlow & Associates, LLC |
| Gregory C. Critchfield, M.D., M.S. | | Co-CEO, EarlyDiagnostics, Inc. |
| Kim Kamdar, Ph.D. | | Partner, Domain Associates, LLC |
| Sandra A.J. Lawrence | | Independent Corporate Director |
| Mansoor Raza Mirza, M.D. | | Chief Oncologist, the Copenhagen University Hospital, Denmark and Medical Director of the Nordic Society of Gynaecological Oncology |
| Joshua Phillips | | Managing Partner, Catalyst Health Ventures |
| Ryan Trimble | | Non-employee director, Sera Prognostics, Inc. |
| Marcus Wilson, Pharm.D. | | Chief Analytics Officer, Elevance Health |
Available Information
Our website address is www.seraprognostics.com. Our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and amendments to reports filed pursuant to Sections 13(a) and 15(d) of the Securities Exchange Act of 1934, as amended, or the Exchange Act, are filed with the SEC. Such reports and other information filed by us with the SEC are available free of charge on our website at investors.seraprognostics.com when such reports are available on the SEC’s website. The SEC maintains an internet site that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC at www.sec.gov. The information contained on the websites referenced in this Form 10-K is not incorporated by reference into this filing. Further, our references to website URLs are intended to be inactive textual references only.
Item 1A. Risk Factors
Investing in our Class A common stock involves a high degree of risk. You should carefully consider the risks and uncertainties described below, the section of this Annual Report on Form 10-K entitled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our financial statements and related notes, before investing in our Class A common stock. The risks and uncertainties described below are not the only ones we face. Additional risks and uncertainties that we are unaware of, or that we currently believe are not material, may also become important factors that affect us. If any of the following risks occur, our business, operating results and prospects could be materially harmed. In that event, the price of our Class A common stock could decline, and you could lose part or all of your investment.
Summary of Risk Factors
Our business is subject to numerous risks and uncertainties, including those highlighted in this section below, that represent challenges that we face in connection with the successful implementation of our strategy. The occurrence of one or more of the events or circumstances described in more detail in the risk factors below, alone or in combination with other events or circumstances, may have an adverse effect on our business, cash flows, financial condition, and results of operations. Such risks include, but are not limited to:
•We have incurred net losses since our inception and we anticipate that we will continue to incur losses for the foreseeable future, which could harm our future business prospects.
•Operating our business requires a significant amount of cash, and our ability to generate sufficient cash depends on many factors, some of which are beyond our control and if we cannot raise additional capital when needed, we may have to curtail or cease operations.
•Our quarterly and annual results may fluctuate from period to period, which could adversely impact the value of our Class A common stock.
•We have derived substantially all of our revenues to date from the PreTRM test, and if our efforts to further increase the use and adoption of the PreTRM test or to develop new products and services in the future do not succeed, our business will be harmed.
•In the near future, we expect to rely on sales to a limited number of direct customers for a significant portion of our revenue and cash flows related to the sale of the PreTRM test, making us subject to customer concentration risk.
•If we are unable to establish and maintain sales and marketing capabilities, we may not be successful in commercializing the PreTRM test.
•Competition in the life science industry, including companies engaged in molecular diagnostics and proteomics, is intense. If we are unable to compete successfully with respect to our current or future products or services, we may not be able to increase or sustain our revenues or achieve profitability.
•If our CLIA-certified laboratory facility becomes inoperable, we will be unable to perform our tests and our business will be harmed.
•Interim, top-line and preliminary data from our clinical trials that we announce or publish from time to time may change as additional data become available and are subject to confirmation, audit, and verification procedures that could result in material changes in the final data.
•Our business would be materially harmed if our proprietary biobank were to become contaminated, lost or destroyed.
•We rely on third parties for specimen collection, including phlebotomy services, and commercial courier delivery services, and if these services are disrupted, our business will be harmed.
•We rely on a limited number of suppliers or, in some cases, single suppliers, for some of our laboratory instruments and materials and may not be able to find replacements or immediately transition to alternative suppliers on a cost-effective basis, or at all.
•Our ability to utilize our net operating loss carryforwards and certain other tax attributes may be limited.
•Our estimates of total addressable market opportunity and forecasts of market growth may prove to be inaccurate, and even if the market in which we compete achieves the forecasted growth, our business could fail to grow at a similar rate.
•The inflationary environment could materially adversely impact our business and results of operations.
•If third-party payers do not adequately reimburse for the PreTRM test or any new tests we may develop, such tests may not be purchased or used, which may adversely affect our revenue and profits.
•New reimbursement methodologies applicable to the PreTRM test, and other future tests, including new CPT codes, may decrease reimbursement rates from third-party payers.
•Billing disputes with third-party payers, including disagreement regarding the selection and use of CPT codes when submitting claims, may decrease realized revenue and may lead to requests for recoupment of past amounts paid.
•When third-party payers deny coverage, we are often unable to collect from the patient or any other source and risk disputes if we attempt to do so.
•Our revenues may be adversely impacted if third-party payers withdraw coverage or provide lower levels of reimbursement due to changing policies, billing complexities or other factors.
•Status as an out-of-network provider with a large commercial insurer may cause health care providers to avoid recommending our tests.
•If the validity of an informed consent from a patient is challenged, we could be precluded from billing for such patient’s testing, be forced to stop performing certain tests, forced to exclude the patient’s data or specimens from clinical trial results or be subject to lawsuits or regulatory enforcement.
•Changes in the way the FDA regulates the reagents, other consumables, and testing equipment we use when developing, validating, and performing our tests could result in delay or additional expense in bringing our tests to market or performing such tests for our customers.
•If we fail to comply with federal and/or state laboratory licensing requirements, we could lose the ability to perform our tests or experience disruptions to our business.
•Any failure to obtain, maintain, and enforce our intellectual property rights could impair our ability to protect our proprietary technology and our brand.
•Issued patents covering our tests and technology could be found invalid or unenforceable, if challenged.
•Our intellectual property may be infringed by a third party.
•If we are not able to prevent disclosure of our trade secrets and other proprietary information, the value of our tests and technology could be significantly diminished.
•The price of our Class A common stock may be volatile, and you could lose all or part of your investment.
•Sales of a substantial number of shares of our Class A common stock by our existing stockholders in the public market could cause our stock price to fall.
•Our inability to maintain effective disclosure controls and procedures could adversely affect our results of operations, liquidity and financial positions, as well as our stock price and investor confidence in us.
Risks Related to Our Financial Position and Need for Additional Capital
We have incurred net losses since our inception and we anticipate that we will continue to incur losses for the foreseeable future, which could harm our future business prospects.
We have incurred net losses each year since our inception in 2008. To date, we have financed our operations primarily through private placements of our equity and debt securities, bank loans and the sale and issuance of Class A common stock in our initial public offering (“IPO”), which was completed in July 2021. Our net loss for the years ended December 31, 2023 and 2022 was $36.2 million and $44.2 million, respectively. As of December 31, 2023, we had an accumulated deficit of $246.9 million. Our losses may continue to increase in the future as we continue to devote a substantial portion of our resources to efforts to increase the adoption of, and reimbursement for, the PreTRM test, make improvements to this product, and research, develop, and commercialize new products.
We currently receive substantially all of our revenues from the sales of the PreTRM test and expect to continue to receive revenue from sales of the PreTRM test and our other pipeline products and services, if approved, in the future. It is possible that we will not generate sufficient revenue from the sales of any of our products and services to cover our costs, including research and development expenses related to furthering our product pipeline, and achieve or sustain profitability. A significant element of our business strategy is to increase and maintain our in-network coverage with third-party payers. However, third-party payers, such as commercial insurers and government health care programs, may decide not to reimburse for the PreTRM test or other tests we may develop, may not reimburse for uses of the PreTRM test or our other tests for the pregnant patient population, or may set the amounts of such reimbursements at prices that do not allow us to cover our expenses. Many third-party payers currently either have negative coverage determinations or otherwise do not reimburse for low-risk patient preterm birth screening tests. State Medicaid programs currently do not reimburse for our tests; third-party payers are increasingly requiring that prior authorization be obtained prior to conducting testing as a condition to reimbursing for it, which may reduce and/or delay the reimbursement amounts.
As there is a possibility that our Company, any collaborators and/or licensees may not successfully develop additional products, obtain required regulatory authorizations for such products, manufacture such products at an acceptable cost or with sufficient quality or successfully market and sell such products with desired margins, our expenses may continue to exceed any revenues we may receive. Our operating expenses also will increase as, or if, among other factors:
•our earlier-stage products move into later-stage development, which is generally more expensive than early-stage development;
•we select additional technologies or products for development;
•we increase the number of patents we are prosecuting or otherwise expend additional resources on patent prosecution or defense; or
•we acquire or in-license additional technologies, product candidates, products or businesses.
Operating our business requires a significant amount of cash, and our ability to generate sufficient cash depends on many factors, some of which are beyond our control and if we cannot raise additional capital when needed, we may have to curtail or cease operations.
In the future, we expect to incur significant costs in connection with our operations, including, but not limited to, the development, marketing authorization, and commercialization of new tests, and other products. These development activities generally require a substantial investment before we can determine commercial viability. We expect to need to raise additional funds through public or private equity or debt financings, collaborations or licensing arrangements to continue to fund or expand our operations.
Our actual liquidity and capital funding requirements will depend on numerous factors, including:
•our ability to achieve broad commercial success with the PreTRM test and other pipeline products and services;
•the scope and duration of, and expenditures associated with, our discovery efforts and research and development programs, including for our proprietary proteomics and bioinformatics platform;
•the costs to fund our commercialization strategies for any product candidates which we launch and to prepare for potential product marketing authorizations, as required;
•the costs of any acquisitions of complementary businesses or technologies that we may pursue;
•potential licensing or partnering transactions, if any;
•our facility expenses, which will vary depending on the time and terms of any facility lease or sublease we may enter into, and other operating expenses;
•the scope and extent of the expansion of our sales and marketing efforts;
•the commercial success of our other products and services;
•our ability to obtain more extensive coverage and reimbursement for the PreTRM test and other products and services, if any; and
•our ability to collect our accounts receivable.
The availability of additional capital, whether from private capital sources, such as banks, or the public capital markets, may fluctuate as our financial condition and market conditions in general change. There may be times when the private capital sources and the public capital markets lack sufficient liquidity or when our securities cannot be sold at attractive prices, or at all, in which case we would not be able to access capital from these sources. In addition, any weakening of our financial condition or deterioration in our credit ratings could adversely affect our ability to obtain necessary funds. Even if available, additional financing could be costly or have adverse consequences.
Additional capital, if needed, may not be available on satisfactory terms or at all. Furthermore, any additional capital raised through the sale of equity or equity-linked securities will dilute our stockholders’ ownership interests and may have an adverse effect on the price of our Class A common stock. In addition, the terms of any financing may adversely affect stockholders’ holdings or rights. Debt financing, if available, may include restrictive covenants. To the extent that we raise additional funds through collaborations and licensing arrangements, it may be necessary to relinquish some rights to our technologies or grant licenses on terms that may not be favorable to us.
If we are not able to obtain adequate funding when needed, we may be required to delay development programs or sales and marketing initiatives. If we are unable to raise additional capital in sufficient amounts or on satisfactory terms, we may have to reduce our workforce and may be prevented from continuing our discovery, development and commercialization efforts and leveraging other corporate opportunities. In addition, it may be necessary to work with a partner on one or more of our tests or products under development, which could lower our economic value of those products. Each of the foregoing factors may harm our business, operating results, and financial condition and may impact our ability to continue as a going concern.
Adverse developments affecting the financial services industry, such as actual events or concerns involving liquidity, defaults or non-performance by financial institutions or transactional counterparties, could adversely affect our current and projected business operations and our financial condition and results of operations.
Actual events involving limited liquidity, defaults, non-performance or other adverse developments that affect financial institutions, transactional counterparties or other companies in the financial services industry or the financial services industry generally, or concerns or rumors about any events of these kinds or other similar risks, have in the past and may in the future lead to market-wide liquidity problems. For example, on March 10, 2023, Silicon Valley Bank, or SVB, was closed by the California Department of Financial Protection and Innovation, which appointed the Federal Deposit Insurance Corporation, or the FDIC, as receiver. Similarly, on March 12, 2023, Signature Bank and Silvergate Capital Corp. were each swept into receivership. In addition, on May 1, 2023, the FDIC announced that First Republic had been closed by the California Department of Financial Protection and Innovation and its assets seized by the FDIC. If any of our partners, suppliers, or other parties with whom we conduct business are unable to access funds pursuant to such instruments or lending arrangements with such a financial institution, such parties’ ability to pay their obligations to us or to enter into new commercial arrangements requiring additional payments to us could be adversely affected. Similar impacts have occurred in the past, such as during the 2008-2010 financial crisis.
Inflation and rapid increases in interest rates have led to a decline in the trading value of previously issued government securities with interest rates below current market interest rates. Although the U.S. Department of Treasury, FDIC and Federal Reserve Board have announced a program to provide up to $25 billion of loans to financial institutions secured by certain of such government securities held by financial institutions to mitigate the risk of potential losses on the sale of such instruments, widespread demands for customer withdrawals or other liquidity needs of financial institutions for immediate liquidity may exceed the capacity of such program. There is no guarantee that the U.S. Department of Treasury, FDIC and Federal Reserve Board will provide access to uninsured funds in the future in the event of the closure of other banks or financial institutions, or that they would do so in a timely fashion.
Although we assess our banking relationships as we believe necessary or appropriate, our access to funding sources and other credit arrangements in amounts adequate to finance or capitalize our current and projected future business operations could be significantly impaired by factors that affect us, the financial institutions with which we have arrangements directly, or the financial services industry or economy in general. These factors could include, among others, events such as liquidity constraints or failures, the ability to perform obligations under various types of financial, credit or liquidity agreements or arrangements, disruptions or instability in the financial services industry or financial markets, or concerns or negative expectations about the prospects for companies in the financial services industry. These factors could involve financial institutions or financial services industry companies with which we have financial or business relationships, but could also include factors involving financial markets or the financial services industry generally.
The results of events or concerns that involve one or more of these factors could include a variety of material and adverse impacts on our current and projected business operations and our financial condition and results of operations. These could include, but may not be limited to, the following:
•Delayed access to deposits or other financial assets or the uninsured loss of deposits or other financial assets;
•Loss of access to revolving existing credit facilities or other working capital sources and/or the inability to refund, roll over or extend the maturity of, or enter into new credit facilities or other working capital resources;
•Potential or actual breach of contractual obligations that require us to maintain letters or credit or other credit support arrangements; or
•Termination of cash management arrangements and/or delays in accessing or actual loss of funds subject to cash management arrangements.
In addition, investor concerns regarding the U.S. or international financial systems could result in less favorable commercial financing terms, including higher interest rates or costs and tighter financial and operating covenants, or systemic limitations on access to credit and liquidity sources, thereby making it more difficult for us to acquire financing on acceptable terms or at all. Any decline in available funding or access to our cash and liquidity resources could, among other risks, adversely impact our ability to meet our operating expenses, financial obligations or fulfill our other obligations, result in breaches of our financial and/or contractual obligations or result in violations of federal or state wage and hour laws. Any of these impacts, or any other impacts resulting from the factors described above or other related or similar factors not described above, could have material adverse impacts on our liquidity and our current and/or projected business operations and financial condition and results of operations.
In addition, any further deterioration in the macroeconomic landscape or financial services industry could lead to losses or defaults by parties with whom we conduct business, which in turn, could have a material adverse effect on our current and/or projected business operations and results of operations and financial condition.
Our quarterly and annual results may fluctuate from period to period, which could adversely impact the value of our Class A common stock.
Our quarterly and annual results of operations, including our revenues, gross margin, net loss, and cash flows, may vary from period to period as a result of a variety of factors, many of which are outside of our control, including those listed elsewhere in this “Risk Factors” section, and as a result, period-to-period comparisons of our operating results may not be meaningful. Our quarterly and annual results should not be relied upon as an indication of future performance. In addition, to the extent that we continue to spend considerably on our internal sales and marketing and research and development efforts, we expect to incur costs in advance of achieving the anticipated benefits of such efforts. We also face competitive pricing and reimbursement pressures, and we may not be able to maintain our premium pricing in the future, which would adversely affect our operating results. Fluctuations in quarterly and annual results and key metrics may cause our results to fall below our financial guidance, if any, or other projections or goals, or the expectations of analysts or investors, which could adversely affect the price of our Class A common stock.
As a result of our failure to timely file a Current Report on Form 8-K, we are currently ineligible to file new short form registration statements on Form S-3, which may impair our ability to raise capital on terms favorable to us, in a timely manner or at all.
Form S-3 permits eligible issuers to conduct registered offerings using a short form registration statement that allows the issuer to incorporate by reference its past and future filings and reports made under the Exchange Act. In addition, Form S-3 enables eligible issuers to conduct primary offerings “off the shelf” under Rule 415 of the Securities Act. The shelf registration process, combined with the ability to forward incorporate information, allows issuers to avoid delays and interruptions in the offering process and to access the capital markets in a more expeditious and efficient manner than raising capital in a standard registered offering pursuant to a Registration Statement on Form S-1. The ability to register securities for resale may also be limited as a result of the loss of Form S-3 eligibility.
As a result of our failure to timely file a Current Report on Form 8-K, we are currently ineligible to file new short form registration statements on Form S-3 until June 2024. Our inability to use Form S-3 may impair our ability to raise necessary capital to fund our operations and execute our strategy. If we seek to access the capital markets through a registered offering during the period of time that we are unable to use Form S-3, we may be required to publicly disclose the proposed offering and the material terms thereof before the offering commences, we may experience delays in the
offering process due to SEC review of a Form S-1 registration statement and we may incur increased offering and transaction costs and other considerations. Disclosing a public offering prior to the formal commencement of an offering may result in downward pressure on our share price. If we are unable to raise capital through a registered offering, we would be required to conduct our equity financing transactions on a private placement basis, which may be subject to pricing, size and other limitations imposed under the Nasdaq rules, or seek other sources of capital. The foregoing limitations on our financing approaches could have a material adverse effect on our results of operations, liquidity, and financial position.
Risks Related to Our Business and Industry
We have derived substantially all of our revenues to date from the PreTRM test, and if our efforts to further increase the use and adoption of the PreTRM test or to develop new products and services in the future do not succeed, our business will be harmed.
We currently receive and expect to continue to receive substantially all of our revenues from the sales of the PreTRM test in the near term. We intend to establish reimbursement for the PreTRM test by collaborating with payers to perform rigorous analysis to demonstrate the health and economic benefits of our biomarker tests within their own network using customized inputs based on the plan’s patient population. We plan to leverage early payer reimbursement decisions to obtain widespread commercial coverage of the PreTRM test from many regional and national plans and medical groups with doctors ordering the PreTRM test. If we are unable to execute on this commercial strategy and increase our revenues from the sale of the PreTRM test, our business may be materially adversely impacted. Our ability to increase sales of the PreTRM test and establish greater levels of adoption and reimbursement for the PreTRM test is uncertain for many reasons, including, among others:
•we may be unable to demonstrate to clinics, clinicians, physicians, payers, and patients that the PreTRM test is superior to alternatives with respect to value, convenience, accuracy, scope of coverage, and other factors;
•third-party payers may set the amounts of reimbursement at prices that reduce our profit margins or do not allow us to cover our expenses;
•we may not be able to maintain and grow effective sales and marketing capabilities;
•our sales and marketing efforts may fail to effectively reach customers or communicate the benefits of the PreTRM test;
•superior alternatives to the PreTRM test may be developed and commercialized and we may not be able to compete against these alternatives;
•we may face competitive pressures;
•we may experience supply constraints, including due to the failure of our key suppliers to provide laboratory supplies, instruments, and reagents;
•we may encounter difficulties with transportation logistics, regulations and quality associated with shipping blood specimens, including infrastructure conditions, transportation delays and temperature stress;
•we may encounter laboratory process difficulties that impact the quality and timeliness of reporting of test results;
•U.S. or foreign regulatory or legislative bodies may adopt new regulations or policies or take other actions that impose significant restrictions on, or other challenges to, our ability to sell or market our products;
•news media organizations, medical societies, or industry groups may issue publications, guidance, or analyses that negatively impact patients’ and/or health care providers’ perception or utilization of the PreTRM test (or certain types of prenatal testing and related health care services, generally) and thereby negatively impact our ability to sell or market the PreTRM test;
•we may be unable to compete successfully with respect to our current or future products or services, as a result of which we may not be able to increase or sustain our revenues or achieve profitability; and
•we may not be able to protect our intellectual property position.
If our market share for the PreTRM test fails to grow or grows more slowly than expected, or if our efforts to develop new products and services in the future do not succeed, our business, operating results, and financial condition would be adversely affected.
Our success depends on broad scientific and market acceptance of the PreTRM test and our other pipeline products and services, which we may fail to achieve.
Our ability to achieve and maintain scientific and commercial market acceptance of the PreTRM test will depend on a number of factors. We expect that the PreTRM test will be subject to the market forces and adoption curves common to other new technologies. The market for proteomics and bioinformatics technologies and products is in its early stages of development. If widespread adoption of the PreTRM test or any other products that we commercialize in the future takes longer than anticipated, we will continue to experience operating losses. The success of life sciences technologies and products is due, in large part, to acceptance by the scientific and medical communities and their adoption of certain products in the applicable field of research. The life sciences scientific community is often led by a small number of early adopters and key opinion leaders who significantly influence the rest of the community through publications in peer-reviewed journals. In such journal publications, the researchers will describe their discoveries, and also the methods, and typically the products used, to fuel such discoveries. Mentions in peer-reviewed journal publications may be a driver for the general acceptance of products for the life sciences industry, such as the PreTRM test. In addition, continuing collaborative relationships with opinion leaders will be vital to maintaining any market acceptance we achieve. If too few researchers describe the use of our products, too many researchers shift to a competing product and publish research outlining their use of that product, or too many researchers negatively describe the use of our products in publications, it may drive customers away from our products. Other factors in achieving commercial market acceptance include:
•our ability to market and increase awareness of the capabilities of the PreTRM test;
•the ability of the PreTRM test to demonstrate comparable performance in intended use applications broadly in the hands of customers;
•our customers’ willingness to adopt new products and workflows;
•the PreTRM test’s ease of use and whether it reliably provides advantages over other alternative technologies;
•the rate of adoption of the PreTRM test by patients, physicians, payers and the medical community at large;
•medical society guidelines supporting the use of the PreTRM test and clinical interventions based on it;
•the prices we charge for the PreTRM test;
•our ability to develop new products and solutions for customers;
•whether competitors develop and commercialize products that perform similar functions as the PreTRM test; and
•the impact of our investments in product innovation and commercial growth.
We cannot assure that we will be successful in addressing each of these criteria or other criteria that might affect the market acceptance of any products we commercialize, particularly the PreTRM test. If we are unsuccessful in achieving and maintaining market acceptance of the PreTRM test, our business, financial condition, and results of operations would be adversely affected.
In the near future, we expect to rely on sales to a limited number of direct customers for a significant portion of our revenue and cash flows related to the sale of the PreTRM test, making us subject to customer concentration risk.
We expect that a significant portion of our revenue and cash flows in the near future will be related to sales to a limited number of customers, including Elevance Health, the loss of any of which could adversely affect our business, financial condition, cash flows, and results of operations. Accordingly, we are subject to customer concentration risk. Furthermore, any termination of our relationship with Elevance Health would also adversely impact our strategy to rapidly accelerate commercialization of the PreTRM test and help incentivize broader market adoption.
If we are unable to establish and maintain sales and marketing capabilities, we may not be successful in commercializing the PreTRM test.
We have limited experience as a company in sales and marketing and our ability to achieve profitability depends on our being able to attract customers for the PreTRM test and our future products, once approved. Although members of our management team have considerable industry experience, successfully commercializing the PreTRM test will require adapting our sales, marketing, distribution, and customer service and support capabilities to current and ever-changing
market conditions. To perform sales, marketing, distribution, and customer service and support successfully, we will face a number of risks, including:
•our ability to attract, retain, and manage the sales, marketing, and customer service and operations workforce necessary to commercialize and gain market acceptance for our technology;
•the time and cost of establishing a specialized sales, marketing, and customer service and operations workforce; and
•our sales, marketing, and customer service and support team may be unable to initiate and execute successful commercialization activities.
We may seek to enlist one or more third parties to assist with sales, distribution, and customer service and support. There is no guarantee, if we do seek to enter into such arrangements, that we will be successful in attracting desirable sales and distribution partners or that we will be able to enter into such arrangements on favorable terms. If our sales and marketing efforts, or those of any third-party sales and distribution partners, are not successful, the PreTRM test may not gain market acceptance, which could materially impact our business operations.
Even if the PreTRM test achieves broad scientific and market acceptance, if we fail to improve it or introduce compelling new products, our future revenues and prospects could be harmed.
Even if we are able to achieve broad scientific and market acceptance for the PreTRM test, our ability to grow our business will depend in large part on our ability both to enhance and improve the PreTRM test and to introduce compelling new products, including for major pregnancy related conditions beyond preterm birth. The success of any enhancement to the PreTRM test or introduction of new products depends on several factors, including completion of certain clinical development requirements, timely completion and delivery of the product, competitive pricing, adequate quality testing, integration with existing technologies, appropriately timed and staged product introductions, and overall market acceptance. Any new product or enhancement to the PreTRM test that we develop may not be introduced in a timely or cost-effective manner, may contain defects, errors or vulnerabilities or may not achieve the market acceptance necessary to generate significant revenue.
The typical development cycle of new life sciences products can be lengthy and complicated and may require new scientific discoveries or advancements, considerable resources, and complex technology and engineering. Such developments may involve external suppliers and service providers, making the management of development projects complex and subject to risks and uncertainties regarding timing, timely delivery of required components or services and satisfactory technical performance of such components or assembled products. If we do not achieve the required technical specifications or successfully manage new product development processes, or if development work is not performed according to schedule, then such new technologies or products may be adversely impacted. To date, we have only completed the development process for one product. We cannot assure you that we will ever succeed in completing that process for another product, including for major pregnancy related conditions beyond preterm birth, or that even if we do, it will be launched successfully in the market and find commercial acceptance. If we are unable to successfully develop new products, enhance the PreTRM test to meet customer requirements, compete with alternative products or otherwise gain and maintain market acceptance, our business, results of operations, and financial condition could be harmed.
Competition in the life science industry, including companies engaged in molecular diagnostics and proteomics, is intense. If we are unable to compete successfully with respect to our current or future products or services, we may not be able to increase or sustain our revenues or achieve profitability.
We are a women’s health diagnostic company utilizing our proprietary proteomics and bioinformatics platform to discover, develop, and commercialize biomarker tests, and our first commercial product, the PreTRM test, is designed to accurately predict the risk of premature delivery. The proteomics and bioinformatics industry is characterized by rapid technological changes, frequent new product introductions, reimbursement challenges, emerging competition, intellectual property disputes and litigation, price competition, aggressive marketing practices, evolving industry standards and changing customer preferences. We cannot guarantee that research, discoveries or other advancements by other companies will not render our existing or potential products and services uneconomical or result in products and services that are superior or otherwise preferable to our current or future products and services.
We face competition with respect to the PreTRM test and expect to face competition with respect to any product candidates that we may seek to develop or commercialize in the future. Many of the companies against which we are competing or may compete against in the future have significantly greater financial resources and expertise in research and
development, manufacturing, and commercialization. Mergers and acquisitions in our industry may result in even more resources being concentrated among a smaller number of our competitors. Smaller and early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These third parties compete with us in recruiting and retaining qualified scientific and management personnel and conducting clinical trials, as well as in acquiring technologies complementary to, or necessary for, our products and services.
To remain competitive over time, we will need to continually research and develop improvements to our products and services. However, we cannot assure you that we will be able to develop and commercialize any improvements to our products and services on a timely basis. Our competitors may develop and commercialize competing or alternative products and services and improvements faster than we are able to do so, which would negatively affect our ability to increase or sustain our revenue or achieve profitability.
If our products do not perform as expected, our operating results, reputation, and business will suffer.
Our success depends on the market’s confidence that we can provide reliable, high-quality testing results. There is no guarantee that the accuracy and reproducibility we have demonstrated to date will continue as our test volumes continue to increase and our product portfolio continues to expand. We believe that patients that rely on our tests are particularly sensitive to test limitations and errors, including inaccurate test results. As a result, if our tests do not perform as expected or favorably in comparison to competing tests, our operating results, reputation, and business will suffer. We may also become subject to legal claims arising from such limitations, errors or inaccuracies.
The PreTRM test uses, and our future tests will use, a number of complex and sophisticated proteomic and bioinformatics processes and advanced mass spectrometry techniques, which are highly sensitive to external factors. An operational, technological or other failure in one of these complex processes may result in sensitivity or specificity rates that are lower than we anticipate. In addition, we regularly evaluate and refine our testing processes, and any refinements we make may not improve our tests as we expect and may result in unanticipated issues that may adversely affect our test performance as described above. Such operational, technical, and other difficulties adversely affect test performance, may impact the commercial attractiveness of our products and may increase our costs or divert our resources, including management’s time and attention, from other projects and priorities. Furthermore, any changes to our testing process may require us to use new or different suppliers or materials with whom or which we are unfamiliar, and which may not perform as we anticipate, and could cause delays, downtime or other operational issues.
If our CLIA-certified laboratory facility becomes inoperable, we will be unable to perform our tests and our business will be harmed.
We currently operate a CLIA-certified laboratory facility in Salt Lake City, Utah, which processes the PreTRM test and likely any other future test, if approved, that is or will be the source of substantially all of our revenues. Our facility could be harmed or rendered inoperable, or our supplies or other assets could be damaged or destroyed, by natural or man-made disasters, including earthquakes, severe weather, flooding, power outages, and contamination, including as a result of a public health threat, which may render it difficult or impossible for us to operate our business and/or perform our tests for some period of time. The inability to perform our tests or the backlog of tests that could develop if our facility is inoperable — for even a short period of time — may harm our reputation and result in a material adverse effect on our revenues.
The marketing, sale, and use of the PreTRM test and any other products that we develop in the future could result in substantial damages arising from product liability or professional liability claims, associated with product recalls or otherwise, that exceed our resources.
The marketing, sale, and use of the PreTRM test and any other products that we develop and commercialize in the future could lead to product liability claims against us if someone were to allege that the PreTRM test or any future product failed to perform as it was designed or as claimed in our promotional materials, was performed pursuant to incorrect or inadequate laboratory procedures, if we delivered incorrect or incomplete test results or if someone were to misinterpret test results. In addition, we may be subject to liability for errors in, a misunderstanding of, or inappropriate reliance upon, the information we provide, or for failure to provide such information, in connection with our marketing and promotional activities or as part of the results generated by the PreTRM test and other future products or services. Even though the PreTRM test is highly accurate, no test is 100% accurate, and we may report false results. In such a scenario, the patient or her family may file a lawsuit against us claiming product or professional liability. In addition, any manufacturing or design
defects in our products could lead to product recalls, either voluntary or as required by government authorities, which could result in the removal of a product from the market.
A product liability or professional liability claim could result in substantial damages and be costly and time-consuming for us to defend. Although we maintain product and professional liability insurance, our insurance may not fully protect us from the financial impact of defending against product liability or professional liability claims or any judgments, fines or settlement costs arising out of any such claims, or the financial and reputational consequences of a product recall. Any product liability or professional liability claim brought against us, with or without merit, could increase our insurance rates, cause our insurance coverage to be terminated or prevent us from securing insurance coverage in the future. As we attempt to bring new products to market, we may need to increase our product liability coverage, which would be a significant additional expense that we may not be able to afford. Additionally, any product liability or professional liability lawsuit could harm our reputation, result in a cessation of PreTRM testing or cause our partners to terminate our agreements with them, any of which could adversely impact our results of operations.
The results of our clinical trials and studies may not support the use of our tests and other product candidates, or may not be replicated in later studies.
We have conducted and are currently conducting a variety of observational and interventional studies for the PreTRM test and our other tests in development that involve clinical investigators at multiple sites in the United States. We may need to conduct additional studies for the PreTRM test, as well as other tests we may offer in the future, to drive test adoption in the marketplace and reimbursement. Should we not be able to perform these studies, or should their results not provide clinically meaningful data and value for clinicians, or if our results are unfavorable, adoption of our tests could be impaired.
The administration of clinical and economic utility studies is expensive and demands significant attention from certain members of our management team. Data collected from these studies may not be positive or consistent with our existing data, or may not be statistically significant or compelling to the medical community or payers. If the results obtained from our ongoing or future studies are inconsistent with certain results obtained from our previous studies, adoption of our products would suffer and our business would be harmed.
Peer-reviewed publications regarding our products and product candidates may be limited by many factors, including delays in the completion of, poor design of, or lack of compelling data from clinical studies, as well as delays in the review, acceptance, and publication process. If our products or product candidates or the technology underlying our current or future products or product candidates do not receive sufficient favorable exposure in peer-reviewed publications, or are not published, the rate of health care provider adoption of our tests and positive reimbursement coverage decisions for our tests and other products could be negatively affected. The publication of clinical data in peer-reviewed journals can be a crucial step in commercializing and obtaining reimbursement for tests, and our inability to control when, if ever, results are published may delay or limit our ability to derive sufficient revenues from any test that is the subject of a study. The performance achieved in published studies may not be repeated in later studies that may be required to obtain FDA marketing authorizations should we decide to do so for business reasons, or should we be required to submit applications to the FDA or other health authorities seeking such authorizations.
In addition, clinical trials must be conducted in accordance with applicable laws and subject to the oversight of Institutional Review Boards, or IRBs. We rely on clinical trial sites to ensure the proper and timely conduct of our clinical trials and while we have agreements governing their committed activities, we have limited influence over their actual performance. We depend on our collaborators and on medical institutions to conduct our clinical trials in compliance with applicable human subject protection regulations and Good Clinical Practice, or GCP, requirements. To the extent our collaborators fail to enroll participants for our clinical trials, fail to conduct our trials in compliance with applicable law and GCP requirements, or are delayed for a significant time in the execution of trials, including achieving full enrollment, we may be affected by increased costs, program delays, or both.
Interim, top-line and preliminary data from our clinical trials that we announce or publish from time to time may change as additional data become available and are subject to confirmation, audit, and verification procedures that could result in material changes in the final data.
From time to time, we may publicly disclose interim, top-line or preliminary data from our clinical trials, which is based on a preliminary analysis of then-available data, and these results and related findings and conclusions may be subject to change following a more comprehensive review of the data. We also make assumptions, estimations,
calculations, and conclusions as part of our analyses of data, and we may not have received or have had the opportunity to fully and carefully evaluate all data. As a result, the interim, top-line or preliminary data that we report may differ from future results of the same trials, or different conclusions or considerations may qualify such results once additional data have been received and fully evaluated. Interim data from clinical trials are subject to the risk that one or more of the clinical outcomes may materially change as patient enrollment continues and more patient data become available. Preliminary, interim or top-line data also remain subject to audit and verification procedures that may result in the final data being materially different from the preliminary top-line data we previously published. As a result, preliminary, interim, and top-line data should be viewed with caution until the final data are available. Adverse differences between preliminary, interim, and top-line data and final data could significantly harm our business prospects and may cause the price of our Class A common stock to fluctuate or decline.
Further, payers, physicians, and others may not accept or agree with our assumptions, estimates, calculations, conclusions or analyses or may interpret or weigh the importance of data differently, which could adversely impact the potential of the particular product or program, the prospects for commercialization of any product, and the business prospects of our Company in general. In addition, the information we choose to publicly disclose regarding a particular study or clinical trial is derived from information that is typically extensive, and you or others may not agree with what we determine is material or otherwise appropriate information to include in our disclosure.
If the preliminary, interim or top-line data that we report differ from later or final results, or if payers, physicians or others disagree with the conclusions reached, our ability to commercialize our product candidates may be significantly impaired, which could materially harm our business, operating results, prospects or financial condition.
Our business would be materially harmed if our proprietary biobank were to become contaminated, lost or destroyed.
A fundamental component of our platform is our proprietary biobank, consisting of comprehensive, clinically and demographically annotated blood specimens collected from thousands of pregnant U.S. women, representing the broad demographic and geographic diversity inherent in the U.S. population. This biobank is maintained at our facility in Salt Lake City, Utah, in a secure environment. If the specimens and information contained in the biobank were to become compromised or destroyed, through contamination, theft, a cybersecurity breach, a natural disaster or otherwise, our ability to rely on the data represented in the biobank could be significantly impaired, which could materially harm our business, operating results, prospects or financial condition.
International expansion of our business will expose us to business, regulatory, political, operational, financial, and economic risks associated with doing business outside the United States.
To the extent that we decide to market our products and services outside the United States, our business will be subject to the risks associated with doing business outside the United States, including an increase in our expenses and diversion of our management’s attention from the development of future products and services. Accordingly, our business and financial results in the future could be adversely affected due to a variety of factors, including:
•multiple, conflicting and changing laws and regulations such as data privacy, information security, and data use regulations, tax laws, export and import restrictions, economic sanctions and embargoes, employment laws, anti-corruption laws, regulatory requirements, reimbursement or payer regimes and other governmental approvals, permits, and licenses;
•failure by us or our distributors to obtain any necessary regulatory clearance, authorization or approval for the use of our products and services in various countries;
•additional potentially relevant third-party patent rights;
•complexities and difficulties in obtaining intellectual property protection and maintaining, defending, and enforcing our intellectual property outside the United States;
•difficulties in staffing and managing foreign operations;
•employment risks related to hiring employees outside the United States;
•complexities associated with managing multiple payer reimbursement regimes, government payers or patient self-pay systems;
•difficulties in negotiating favorable reimbursement negotiations with governmental authorities;
•logistics and regulations associated with shipping specimens, including infrastructure conditions and transportation delays;
•limits in our ability to penetrate international markets if we are not able to sell our products or conduct services locally;
•financial risks, such as longer payment cycles, difficulty collecting accounts receivable, the impact of local and regional financial crises on demand and payment for our products and services and exposure to foreign currency exchange rate fluctuations;
•natural disasters, political and economic instability, including wars, terrorism, and political unrest, outbreak of disease, boycotts, curtailment of trade, and other business restrictions;
•regulatory and compliance risks that relate to maintaining accurate information and control over sales and distributors’ activities that may fall within the purview of the U.S. Foreign Corrupt Practices Act, or FCPA, its books and records provisions, or its anti-bribery provisions, or laws similar to the FCPA in other jurisdictions in which we may operate, such as the United Kingdom Bribery Act of 2010, or the U.K. Bribery Act; and
•onerous anti-bribery requirements of several member states in the European Union, the United Kingdom, Japan, and other countries that are constantly changing and require disclosure of information to which U.S. legal privilege may not extend.
Any of these factors could significantly harm our future international expansion and operations and, consequently, our revenue and results of operations.
We may not be able to obtain and maintain the third-party relationships that are necessary to develop and commercialize some or all of our tests.
We expect to depend on collaborators, partners, licensees, and other third parties to support our test development and validation efforts, to deliver needed supplies, and to transport specimens for testing, among other things. Any problems we experience with any of these third parties could delay the development, validation, commercialization, and performance of our testing, which could harm our results of operations.
We cannot guarantee that we will be able to successfully negotiate agreements for, or maintain relationships with, collaborators, partners, licensees, and other third parties on favorable terms, if at all. If we are unable to obtain or maintain these agreements, we may not be able to develop, validate, obtain regulatory authorizations for, or commercialize any future tests, which will in turn adversely affect our business.
We expect to expend substantial management time and effort to enter into relationships with third parties and, if we successfully enter into such relationships, to manage these relationships. In addition, substantial amounts will be paid to third parties in these relationships. However, we cannot control the amount or timing of resources our future contract partners will devote to our business endeavors, and we cannot guarantee that these parties will fulfill their obligations to us under these arrangements in a timely fashion, if at all. In addition, while we manage the relationships with third parties, we cannot control all of the operations of and protection of intellectual property by such third parties.
We rely on third parties for specimen collection, including phlebotomy services, and commercial courier delivery services, and if these services are disrupted, our business will be harmed.
We rely on third parties to perform specimen collection, including phlebotomy services, and to transport specimens to our laboratory facility in a timely and cost-efficient manner. Disruptions in these services, whether due to any natural or other disasters, pandemics, acts of war or terrorism, shipping embargoes, labor unrest, political instability or similar events could adversely affect specimen integrity and our ability to process specimens in a timely manner and to service our customers, and ultimately our reputation and our business. In addition, if we are unable to continue to obtain expedited delivery services on commercially reasonable terms, our operating results may be adversely affected.
In addition, our relationships with these service providers could be scrutinized under federal and state health care laws such as the federal Anti-Kickback Statute and the Stark Law, and their implementing regulations, to the extent, for example, that these services provide a financial benefit to or relieve a financial burden for a potential referral source. If our operations are found to be in violation of any of these (or other) laws and regulations, we may be subject to administrative, civil and/or criminal penalties, damages, fines, individual imprisonment, refunding of payments received by us, exclusion
from government health care programs, and/or curtailment or cessation of our operations, among other potential penalties, any of which could harm our reputation and adversely affect our business, operating results, and financial condition.
We rely on a limited number of suppliers or, in some cases, single suppliers, for some of our laboratory instruments and materials and may not be able to find replacements or immediately transition to alternative suppliers on a cost-effective basis, or at all.
We source components of our technology from third parties and certain components are sole sourced. Obtaining substitute components may be difficult or require us to re-design our products. We expect to continue to depend on third-party contract suppliers for the foreseeable future. Any natural or other disasters, pandemics, acts of war or terrorism, shipping embargoes, labor unrest or political instability or similar events at our third-party suppliers’ facilities that cause a loss of manufacturing capacity or a reduction in the quality of the items manufactured would heighten the risks that we face. In addition, inflation and/or global supply chain disruptions may have a negative impact on our third-party contract suppliers’ ability to acquire the materials necessary for our business and we could incur higher costs for certain goods or services due to inflation or increased freight costs. Changes to, failure to renew or termination of our existing agreements or our inability to enter into new agreements with other suppliers could result in the loss of access to important components of our tests and could impair, delay or suspend our commercialization efforts. Our failure to maintain a continued and cost-effective supply of high-quality components could materially and adversely harm our business, operating results, and financial condition.
If we are unable to successfully scale our operations, or attract and retain highly skilled employees, our business could suffer.
As our test volumes grow and we develop future product offerings, we will need to continue to ramp up our testing capacity and implement increases in scale, such as increased headcount, additional or upgraded equipment, additional qualified laboratory personnel, increased office and laboratory space, expanded customer service capabilities, improved billing and systems processes, enhanced controls and procedures and expanded or internal quality assurance program and technology platform. The value of the PreTRM test and our other testing products that we may develop in the future depends on our ability to perform, and our reputation for performing, these tests on a timely basis and with an exceptionally high standard of quality. Failure to implement necessary procedures, transition to new facilities, purchase and maintain equipment, establish processes, or hire the necessary personnel in a timely and effective manner could result in higher processing costs or an inability to meet market demand or could otherwise affect our operating results.
To execute our growth plan, we must attract and retain highly qualified personnel. Competition for these personnel is intense, especially for sales, scientific, medical, laboratory, research and development, and other technical personnel. The turnover rate of such personnel can be high. We may, from time to time, experience difficulty in hiring and retaining employees with appropriate qualifications. Furthermore, replacing executive officers and key employees may be difficult and may take an extended period of time due to the limited number of individuals in our industry with the breadth of skills and experience required to successfully develop, gain regulatory approval of, and commercialize products. Competition to hire from the limited pool referred to above is intense, and we may be unable to hire, train, retain, or motivate these key personnel on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel. Many of the companies with which we compete for highly qualified personnel have greater resources than we have. If we hire employees from competitors or other companies, their former employers may attempt to assert that these employees or our Company have breached their legal obligations to their former employers, which occurs from time to time. Furthermore, to the extent that we are unable to retain our employees and they leave our Company to join one of our competitors, we cannot assure you that any invention, non-disclosure or non-compete agreements we have in place will provide meaningful protection against a departing employee’s unauthorized use or disclosure of our confidential information.
In addition, our growth may place a significant strain on our operating and financial systems and our management, sales, marketing, and administrative resources. As a result of our growth, our operating costs may escalate faster than we anticipate, we may face difficulties in obtaining additional office or laboratory space and some of our internal systems may need to be enhanced or replaced. If we cannot effectively manage our expanding operations and our costs, we may not be able to grow successfully or we may grow at a slower pace, and our business could be adversely affected.
Any headcount reductions undertaken to extend our cash runway and focus more of our capital resources on our prioritized research and development programs as well as commercialization activities may not achieve our intended outcome.
From time to time, we have made select headcount reductions to more effectively allocate costs toward a refined focus on those opportunities deemed most promising in the near-term from a product adoption and revenue generation perspective. Such headcount reductions may result in unintended consequences and costs, such as the loss of institutional knowledge and expertise, attrition beyond the intended number of employees, decreased morale among our remaining employees, and the risk that we may not achieve the anticipated benefits of the headcount reductions. In addition, while positions have been eliminated, certain functions necessary to our operations remain, and we may be unsuccessful in distributing the duties and obligations of departed employees among our remaining employees. The headcount reductions could also make it difficult for us to pursue, or prevent us from pursuing, new opportunities and initiatives due to insufficient personnel, or require us to incur additional and unanticipated costs to hire new personnel to pursue such opportunities or initiatives. If we are unable to realize the anticipated benefits from the headcount reductions, or if we experience significant adverse consequences from the headcount reductions, our business, financial condition, and results of operations may be materially adversely affected.
We may engage in acquisitions, dispositions or other strategic transactions that could disrupt our business, cause dilution to our stockholders or reduce our financial resources.
From time to time, we may enter into transactions to acquire or dispose of businesses, products or technologies or to engage in other strategic transactions. Because we have not made any such acquisitions to date, our ability to do so successfully is unproven. Even if we identify suitable transactions, we may not be able to complete such transactions on favorable terms or at all. Any acquisitions or other strategic transactions we consummate may not strengthen our competitive position, and these transactions may be viewed negatively by customers or investors. We may decide to incur debt in connection with an acquisition or issue shares of our common stock or other equity securities to the stockholders of the acquired company, which would cause dilution to our existing stockholders. We could incur losses resulting from such strategic transactions, including undiscovered liabilities of an acquired business that are not covered by any indemnification we may obtain from the seller. In addition, we may not be able to successfully integrate any acquired personnel, technologies, and operations into our existing business in an effective, timely and non-disruptive manner. Any dispositions may also cause us to lose revenue and may not strengthen our financial position. Strategic transactions may also divert management attention from day-to-day responsibilities, increase our expenses, result in accounting charges, and reduce our cash available for operations and other uses. We cannot predict the number, timing or size of future strategic transactions or the effect that any such transactions might have on our operating results.
We may need to raise additional funds through equity or debt financings, corporate collaborations or licensing arrangements to continue to fund or expand our operations. Additional capital, if needed, may not be available on satisfactory terms or at all. Furthermore, any additional capital raised through the sale of equity or equity-linked securities, or grant of equity or equity-linked securities in connection with any debt financing, will dilute stockholders’ ownership interests in us and may have an adverse effect on the price of our Class A common stock. In addition, the terms of any financing may adversely affect stockholders’ holdings or rights. To the extent that we raise capital through collaborations and licensing arrangements, it may be necessary to relinquish some rights to our technologies or grant licenses on terms that may not be favorable to us.
If we are not able to obtain adequate funding when needed, we may have to delay development programs or sales and marketing initiatives. In addition, we may have to work with a partner on one or more of our tests or programs, which could lower the economic value of those programs to our Company.
Public health threats, such as COVID-19, could materially affect our operations, as well as the business or operations of third parties with whom we conduct business. Our business could be adversely affected by the effects of other future public health threats in regions where we, or third parties on which we rely, have significant business operations.
Our business and operations, including, but not limited to, our laboratory operations, sales and marketing efforts, supply chain operations, research and development activities, and fundraising activities, could be adversely affected by public health disruptions in regions where we have business operations, and such health disruptions could cause significant disturbance in the operations of third parties upon whom we rely. As a recent example, in March 2020, the World Health Organization declared the COVID-19 outbreak a pandemic, and the U.S. government imposed restrictions on travel between the United States, Europe, and certain other countries. In the years following the initial outbreak, numerous state
and local jurisdictions, including the jurisdictions where our headquarters and laboratory are located, imposed quarantines, shelter-in-place orders, executive orders, and similar government orders for their residents to control the spread of COVID-19. A new serious public health threat could result in similar restrictions being imposed. The future impact of a public health threat is highly uncertain and subject to change. We cannot predict the full extent of potential delays or impacts on our business, our clinical trials, health care systems or the global economy as a whole.
We cannot ensure that our employees will fully adhere to compliance policies and procedures.
We have implemented and strive to continuously develop and improve compliance policies and procedures intended to train our sales, billing, marketing, and other personnel regarding compliance with state and federal laws applicable to our business. Our efforts to implement appropriate monitoring of compliance with such policies and procedures are likewise ongoing. Despite our compliance policies and procedures, and related training and monitoring, we may experience situations in which employees may have failed to fully adhere to our policies and/or applicable laws in the past or in which they fail to adhere to applicable policies and/or laws in the future. Such failures may subject us to administrative, civil, and criminal actions, penalties, damages, fines, individual imprisonment, exclusion from participation in state and/or federal health care programs, refunding of payments received by us, and curtailment or cessation of our operations. In addition, commercial third-party payers may refuse to provide all or any reimbursement for tests administered, seek repayment from us of amounts previously reimbursed and harm our ability to secure network contracts with third-party payers. Any of the foregoing could adversely affect our revenue, cash flow, and financial condition, and reduce our growth prospects. As of the date hereof, we are not aware of any noncompliance with any state and federal laws applicable to our business.
Our ability to utilize our net operating loss carryforwards and certain other tax attributes may be limited.
We have a significant amount of net operating loss, or NOL, carryforwards that can be used to offset potential future taxable income and related income taxes. As of December 31, 2023, we had federal NOL carryforwards of approximately $211.6 million, of which, $70.3 million, if not utilized, begin to expire in 2028. Approximately $141.3 million of these federal NOLs can be carried forward indefinitely. Under Section 382 of the Internal Revenue Code of 1986, as amended, if a corporation undergoes an “ownership change” (generally defined as a greater than 50% change, by value, in equity ownership over any three-year period), the corporation’s ability to use its pre-change NOL carryforwards and other pre-change tax attributes to offset its post-change income or taxes may be limited. We may experience ownership changes in the future as a result of shifts in our stock ownership, some of which may not be within our control. Our ability to use these carryforwards could be limited if we experience an “ownership change.”
Our estimates of total addressable market opportunity and forecasts of market growth may prove to be inaccurate, and even if the market in which we compete achieves the forecasted growth, our business could fail to grow at a similar rate.
Total addressable market opportunity estimates and growth forecasts are subject to significant uncertainty and are based on assumptions and estimates that may not prove to be accurate. Our publicly announced estimates and forecasts relating to the size and expected growth of our market may prove to be inaccurate. Even if the market in which we compete meets our size estimates and forecasted growth, our business could fail to grow at similar rates.
The inflationary environment could materially adversely impact our business and results of operations.
Our operating results could be materially impacted by changes in the overall macroeconomic environment and other economic factors that impact customer confidence and spending, including capital spending. Changes in economic conditions, supply chain constraints, logistics challenges, labor shortages, global conflicts, and steps taken by governments and central banks, particularly in response to public health threats as well as other stimulus and spending programs, have led to higher inflation, which is likely, in turn, to lead to an increase in costs and may cause changes in fiscal and monetary policy, including increased interest rates. In a higher inflationary environment, we may be unable to raise the prices of our products sufficiently to keep up with the rate of inflation. Impacts from inflationary pressures could be more pronounced and materially adversely impact aspects of our business where revenue streams and cost commitments are linked to contractual agreements that extend further into the future, as we may not be able to quickly or easily adjust pricing, reduce costs, or implement counter measures.
Risks Related to Reimbursement
If third-party payers do not adequately reimburse for the PreTRM test or any new tests we may develop, such tests may not be purchased or used, which may adversely affect our revenue and profits.
In the United States and markets in some other countries, patients generally rely on third-party payers to reimburse all or part of the costs associated with their treatment or tests. Adequate coverage and reimbursement from third-party payers such as federal and state health care programs (e.g., Medicare and Medicaid) and commercial insurers is critical to new product acceptance. Our business depends on our ability to obtain or maintain adequate reimbursement from third-party payers. We expect third-party payers such as commercial insurers to be our most significant source of payment in the near future. In particular, we believe that for our Company to achieve commercial success, it will be necessary to gain acceptance from third-party payers for the PreTRM test, and to obtain positive coverage determinations and favorable reimbursement rates from third-party payers for our tests over time. We do not yet know, however, whether and to what extent certain of our products, including those under development, will be covered or reimbursed. If we are unable to obtain or maintain coverage or adequate reimbursement from, or achieve in-network status with, third-party payers for our existing or future tests or other products, our ability to generate revenues will be limited. For example, health care providers may be reluctant to order our tests or other products due to the possibility that a patient may incur substantial costs if third-party payer coverage or reimbursement is unavailable or insufficient. Such coverage and reimbursement may depend upon a number of factors, including the determination that the test and its use or administration for a particular patient are:
•a covered benefit;
•safe, effective, and medically necessary;
•appropriate for the specific patient;
•supported by guidelines established by the relevant professional societies;
•approved in any states where specific assay approval is necessary;
•cost-effective; and
•neither experimental nor investigational.
In the United States, the Centers for Medicare & Medicaid Services, or CMS, an agency within the United States Department of Health and Human Services, or HHS, and its Medicare Administrative Contractors make decisions regarding Medicare coverage for new tests. Other third-party payers, including commercial insurers, often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates, and both CMS and certain commercial insurers may have sufficient market power to demand significant price reductions.
Obtaining coverage and reimbursement approval for a test from each third-party payer is a time-consuming and costly process that could require us to provide to each payer supporting scientific and clinical information, as well as information about patient insurance eligibility and benefits, and billing. We may not be able to provide data sufficient to satisfy third-party payers that they should cover and pay for the test. There is substantial uncertainty whether any particular payer will cover and reimburse the use of any test incorporating new technology. Even when a payer determines that a test is eligible for reimbursement, the payer may impose coverage limitations that preclude payment under certain circumstances or for certain patient populations. Moreover, eligibility for coverage does not mean that any test will be reimbursed in all cases or at a rate that allows us to make a profit or even cover our costs. Interim payments for new tests, if applicable, may also not be sufficient to cover our costs and may not be made permanent. In addition, some payers may require prior authorization before they will pay for a test. We may also have to engage in lengthy and costly appeals in order to overturn payers’ coverage and reimbursement determinations and ultimately obtain payment. Furthermore, reimbursement rates may vary, for example, according to the use of the test and the clinical setting in which it is used, and may reflect budgetary constraints and/or imperfections in Medicare, Medicaid or other data used to calculate these rates.
There have been, and we expect that there will continue to be, federal and state proposals to constrain expenditures for health care products and services, which may affect payments for our tests. Third-party payers, including the Medicare program, frequently change coverage policies, product and service codes and payment methodologies and reimbursement amounts. Due in part to actions by third-party payers, the health care industry is experiencing a trend toward containing or reducing costs through various means, including lowering reimbursement rates and negotiating reduced payment schedules with service providers for certain products and/or services.
Our inability to promptly obtain coverage and profitable reimbursement rates from third-party payers for our tests could have a material and adverse effect on our business, operating results, and financial condition.
In addition, leading professional societies may not recommend our products or services or may recommend alternatives to our tests, which may provide a basis for third-party payers not to cover or reimburse our tests. In making coverage determinations, third-party payers often rely on practice guidelines issued by professional societies. Test-ordering providers may also rely on such guidelines when deciding whether to order testing for their patients. If any relevant professional societies issue guidelines suggesting, or otherwise make recommendations, that providers not use our tests or instead use alternatives to our tests, payers may make unfavorable coverage and reimbursement decisions and test-ordering providers may not order our tests. Any such outcomes could have a material and adverse effect on our business, operating results, and financial condition.
New reimbursement methodologies applicable to the PreTRM test, and other future tests, including new CPT codes, may decrease reimbursement rates from third-party payers.
Generally, two types of coding systems may be used to describe laboratory testing services: (i) CMS’s Healthcare Common Procedure Coding System, or HCPCS, and (ii) the American Medical Association’s, or AMA, Current Procedural Terminology, or CPT, coding systems. Both coding systems use alphanumeric codes to describe the services at issue. Third-party payers, including Medicare, determine which CPT or HCPCS codes they will cover, as well as the circumstances under which they will (or will not) cover those codes and the amount they will reimburse for each code. In some circumstances (such as when a laboratory becomes an in-network provider with a commercial insurer), the third-party payer will negotiate reimbursement amounts with the provider. We use CPT codes to submit claims to payers for our testing and those payers use those same codes to make payments to us.
One type of CPT code is a Proprietary Laboratory Analysis, or PLA, code. PLA codes describe proprietary clinical laboratory analyses. The AMA has issued a unique CPT® PLA code for the PreTRM test. CMS priced this code at $750 in November 2021. Before the AMA issued a PLA code for the PreTRM test, we submitted claims for reimbursement using CPT codes existing at the time based on the guidance of external coding experts.
We cannot guarantee that we will be able to negotiate favorable rates for our unique code, nor can we guarantee that we will receive reimbursement at all, especially if we are unable to collect and publish additional data and obtain positive coverage determinations for the PreTRM test or our other future tests.
We do not currently have specific CPT codes assigned for any of our other tests under development, and there is a risk that we may not be able to obtain such codes or, if obtained, we may not be able to negotiate favorable rates for such codes.
Finally, third-party payers may not establish positive coverage policies for our tests or adequately reimburse for any CPT code we may use, or seek recoupment for testing previously performed, which is a common occurrence in our industry.
Billing disputes with third-party payers, including disagreement regarding the selection and use of CPT codes when submitting claims, may decrease realized revenue and may lead to requests for recoupment of past amounts paid.
It is possible that payers could dispute our billing or coding from time to time. Payers may likewise seek to recoup reimbursements already paid, and we expect that such disputes and requests for recoupment may arise. Third-party payers may also decide to deny payment or recoup payment for testing that they contend to have been not medically necessary, against their coverage determinations, or for which they have otherwise overpaid. There is also a risk that the CPT codes we previously submitted, are currently submitting, or will submit in the future on claims will be rejected or withdrawn or that third-party payers will seek refunds of amounts that they claim were inappropriately billed based on, for example, the CPT code used, the modifier attached, or the number of units billed. Claims for recoupment require the time and attention of our management and other key personnel, which can be a distraction from operating our business.
If third-party payers deny payment for testing, reimbursement revenue for our testing could decline. If a third-party payer successfully challenges that payment for prior testing was in breach of contract or otherwise contrary to policy or law, they may recoup payment, which amounts could be significant and would impact our operating results and financial condition, and it may decrease reimbursement going forward. We may also decide to negotiate and settle with a third-party payer in order to resolve an allegation of overpayment. Any of these outcomes, including recoupment or reimbursements,
might also require us to restate our financials from a prior period, any of which could have a material and adverse effect on our business, operating results, and financial condition.
Failure to comply with laws and regulations related to submission of claims for our services could result in substantial financial penalties and/or potential civil or criminal liability.
We are subject to a variety of complex federal and state laws and regulations applicable to the submission of claims for payment for our services. If a third-party payer or a regulatory or enforcement agency, or, in some cases, a qui tam relator, believes or alleges that we engaged in improper billing practices—including, but not limited to, not adequately pursuing patient cost share responsibilities or submitting improper CPT codes, multipliers or modifiers on our claims—we may be subject to investigation and/or enforcement actions under federal and/or state law.
Responding to and defending such investigations and/or enforcement actions may require significant time and attention from management and key personnel, include significant expenditures, and result in significant penalties, damages, fees, and reputational harm, all of which could have a material adverse effect on our business, operating results, and financial condition. See “— Risks Related to Government Regulation — If we, or our employees or contractors on our behalf, engage in conduct that violates health care laws, are suspected or accused of engaging in such conduct, or are subject to investigation for actual or alleged such conduct, we could face substantial penalties and damage to our reputation, and our business operations and financial condition could be adversely affected.”
“Most favored nation” provisions in contracts with third-party payers may limit potential for revenue growth and may lead to claims for recoupment.
Some of our contracts with third-party payers may in the future contain “most favored nation” provisions, pursuant to which we typically agree that we will not bill the third-party payer more than we bill any other third-party payer. These contract provisions limit the amount we are able to charge for our products and can negatively impact revenue. We monitor our billing and claims submissions for compliance with these contractual requirements with third-party payers. If we do not successfully manage compliance with these most favored nation provisions, we may be required to forego revenues from some third-party payers or reduce the amount we bill to each third-party payer with a most favored nation clause in its contract that is violated, which would adversely affect our business, operating results, and financial condition. This situation could also subject us to claims for recoupment, which could ultimately result in an obligation to repay amounts previously earned.
When third-party payers deny coverage, we are often unable to collect from the patient or any other source and risk disputes if we attempt to do so.
If a third-party payer denies coverage, or if the patient has a large deductible or co-insurance amount, it may be difficult for us to collect from the patient, and we may not be successful in doing so. If we are in-network, we may be contractually prohibited from seeking payment beyond applicable deductibles, co-insurance, or co-payments from the patient. If we are out-of-network, we may be unable to collect the full amount of a patient’s responsibility, despite our good faith efforts to collect. As a result, we may not always be able to collect the full amount due for our tests if third-party payers deny coverage or cover only a portion of the billed amount or if the patient has a large deductible, which could cause payers to raise questions regarding our billing policies and patient collection practices.
We believe that our practices with respect to billing and collecting patient responsibility amounts are compliant with applicable laws; however, we may in the future receive inquiries from third-party payers regarding our practices in these areas. There is no guarantee that we will be successful in addressing such concerns, and if we are unsuccessful, this may result in a third-party payer deciding to reimburse for our tests at a lower rate or not at all, seeking recoupment of amounts previously paid to us, or bringing legal action to seek reimbursement of previous amounts paid. Any such occurrences could cause reimbursement revenue for our testing, which constitutes the large majority of our revenue, to decline. Additionally, if we were required to make a repayment, such repayment could be significant, which could have a material and adverse effect on our business, operating results, and financial condition.
Our revenues may be adversely impacted if third-party payers withdraw coverage or provide lower levels of reimbursement due to changing policies, billing complexities or other factors.
If we become an in-network provider by entering into an agreement with any of the third-party payers from which we receive reimbursement, this means that we will have an agreement that governs approval or payment terms. However, such a contract would not guarantee reimbursement for all testing we perform.
In addition, the terms of any such agreement may require a physician or qualified practitioner’s signature on test requisitions or require other controls and procedures prior to conducting a test. In particular, third-party payers have been increasingly requiring prior authorization to be obtained prior to conducting a test as a condition to reimbursing for the test. If the payers were to do so for the PreTRM test, it could place a burden on our billing operations and require us to dedicate resources to monitoring that these prior authorization requirements are met. To the extent we or the health care providers ordering our tests do not follow the prior authorization requirements, we may be subject to claims for recoupment of reimbursement amounts previously paid to us, or may not receive some or all of the reimbursement amounts to which we would otherwise be entitled. This may occur in the future, which could have a material and adverse effect on our business, operating results, and financial condition.
If we are considered to be an out-of-network provider, which we expect to be the case with at least some of the largest third-party payers from which we may receive reimbursement in the future, such third-party payers could withdraw coverage and decline to reimburse for our tests, for any reason. They can also impose prior authorization requirements through the terms of the patients’ health plans. Managing reimbursement on a case-by-case basis is time-consuming and contributes to an increase in the number of days it takes us to collect on accounts, which also increases our risk of non-payment. Negotiating reimbursement on a case-by-case basis also typically results in the receipt of reimbursement at a significant discount to the list price of our tests.
Even if we are being reimbursed for our tests, third-party payers may unilaterally review and adjust the rate of reimbursement, require co-payments from patients or stop paying for our tests. Federal and state health care programs as well as commercial insurers continue to increase their efforts to control the cost, utilization, and delivery of health care services by demanding price discounts or rebates and limiting coverage of, and amounts they will pay for, molecular tests. These measures have resulted in reduced payment rates and decreased utilization in the clinical laboratory industry. Because of these cost-containment measures, third-party payers — including those that may reimburse our tests in the future — may reduce, suspend, revoke or discontinue payments or coverage at any time. Reduced reimbursement of our tests may harm our business, operating results, and financial condition.
Billing for clinical laboratory testing services is complex. We perform tests in advance of payment and without certainty as to the outcome of the billing process. In cases where we expect to receive a fixed fee per test due to our reimbursement arrangements, we may nevertheless encounter variable reimbursement, leading to disputes over pricing and billing. Each third-party payer typically has different billing requirements, and the billing requirements of many payers have become increasingly difficult to meet. Among the factors complicating our billing of third-party payers are:
•disparity in coverage among various payers;
•disparity in information and billing requirements among payers, including with respect to prior authorization requirements and procedures and establishing medical necessity; and
•incorrect or missing billing information, which is required to be provided by the ordering health care provider.
These risks related to billing complexities, and the associated uncertainty in obtaining payment for our tests, could harm our business, operating results, and financial condition.
Status as an out-of-network provider with a large commercial insurer may cause health care providers to avoid recommending our tests.
We may be considered to be an out-of-network provider with respect to the large commercial insurers from which we may receive reimbursement in the future. Physician groups and other health care providers may view this negatively and may insist upon only using laboratories that are in-network with their patients’ insurance companies. These types of decisions could reduce our revenue and harm our financial condition.
Changes in government health care policy could increase our costs and negatively impact coverage and reimbursement for our tests by governmental and other third-party payers.
The U.S. government is pursuing health care reform and aiming to reduce health care costs. Government health care policy has been, and will likely continue to be, a topic of extensive legislative and executive activity in the U.S. federal government and many U.S. state governments. As a result, our business could be affected by significant and potentially unanticipated changes in government health care policy, which could in turn substantially impact our revenues, increase costs, and divert management attention from our business strategy. We cannot predict the impact of governmental health care policy changes on our future business, operating results, and financial condition.
In the United States, the Affordable Care Act, or ACA, was signed into law in March 2010 and significantly impacted the U.S. pharmaceutical and medical device industries, including the diagnostics sector, in a number of ways. The ACA restricts insurers from charging higher premiums or denying coverage to individuals with pre-existing conditions, and requires insurers to cover certain preventative services without charging any copayment or coinsurance, including screening for lung, breast, colorectal and cervical cancers. The ACA also created a new system of health insurance “exchanges” designed to make health insurance available to individuals and certain groups through state- or federally-administered marketplaces in addition to existing channels for obtaining health insurance coverage. In connection with such exchanges, certain “essential health benefits” are intended to be made more consistent across plans, setting a baseline coverage level. The states (and the federal government) have some discretion in determining the definition of “essential health benefits” and we do not know whether our tests or other products will fall into a benefit category deemed “essential” for coverage purposes across the plans offered in any or all of the exchanges. If any of our tests are not covered by plans offered in the health insurance exchanges, our business, operating results and financial condition could be adversely affected.
There have been multiple attempts to repeal the ACA or significantly scale back its applicability, as a result of which, certain sections of the ACA have not been fully implemented or were effectively repealed. This could negatively impact reimbursement for our testing, adversely affect our test volumes and adversely affect our business, operating results, and financial condition. However, following several years of litigation in the federal courts, in June 2021, the United States Supreme Court upheld the ACA when it dismissed a legal challenge to the Act’s constitutionality. Further legislative and regulatory changes to federal health care laws and policies remain possible. Future changes or additions to the ACA, the Medicare and Medicaid programs, and changes stemming from other health care reform measures, especially with regard to health care access, financing or other legislation in individual states, could have a material adverse effect on the health care industry in the U.S. The uncertainty around the future of the ACA and other health care legislation, and in particular the impact to reimbursement levels and the number of insured individuals, may lead to delay in the purchasing decisions of our customers.
In addition to the ACA, various health care reform proposals have also emerged from federal and state governments. The Protecting Access to Medicare Act of 2014, or PAMA, for example, introduced a multi-year pricing program for services payable under the Clinical Laboratory Fee Schedule, or CLFS, that is designed to bring Medicare allowable amounts in line with the amounts paid by commercial insurers. The rule issued by CMS to implement PAMA required certain laboratories to report third-party payer rates and test volumes, though these reporting requirements have been delayed.
The implementation of Medicare rates pursuant to PAMA has negatively impacted overall pricing and reimbursement for many clinical laboratory testing services and may do so in the future. Since January 1, 2018, the Medicare payment rate for such tests is equal to the weighted median private payer rate reported to CMS, which for many tests is lower than the previous CLFS payment rates due to the often lower negotiated commercial insurer rates applicable to large commercial laboratories that were required to report data to CMS. Likewise, because commercial insurers often base their pricing for laboratory testing on a percentage of the price set on the CLFS, PAMA has in turn affected rates paid by commercial insurers.
The rates paid by Medicare and other state and federal health care programs have been the subject of controversy in the industry, including a lawsuit by the American Clinical Laboratory Association, and it is unclear whether and to what extent the new rates may change.
Other legislative changes have been proposed and adopted in the United States since the ACA was enacted. For example, the Budget Control Act of 2011, among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion
for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several state and federal health care programs. This includes aggregate reductions of Medicare payments to providers up to 2% per fiscal year, and, due to subsequent legislative amendments, will remain in effect through 2032 unless additional Congressional action is taken (with the exception of a temporary suspension from May 1, 2020 through March 31, 2022 due to the COVID-19 pandemic). As another example, in January 2013, the American Taxpayer Relief Act of 2012 was signed into law, which among other things, increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
We cannot predict whether future health care initiatives will be implemented at the federal or state level or how any such future legislation, regulation, or initiative may affect us. Current or potential future federal legislation and the expansion of government’s role in the U.S. health care industry, as well as changes to the reimbursement amounts paid by third-party payers for our current and future tests, may adversely affect our test volumes and adversely affect our business, operating results, and financial condition.
If the validity of an informed consent from a patient is challenged, we could be precluded from billing for such patient’s testing, be forced to stop performing certain tests, forced to exclude the patient’s data or specimens from clinical trial results or be subject to lawsuits or regulatory enforcement.
We are required to ensure that all clinical data and blood specimens that we receive have been collected from subjects who have provided appropriate informed consent for us to perform our testing, both commercially and in clinical trials. Among other things, in our consent forms, we seek to ensure that the subjects from whom the data and specimens are collected do not retain or have conferred on them any proprietary or commercial rights to the data or any discoveries derived from them. A subject’s informed consent could be challenged in the future, and the informed consent could prove invalid, unlawful or otherwise inadequate for our purposes. Any such findings against us, or our partners, could deny us access to, or force us to stop, testing specimens in a particular territory or could call into question the results of our clinical trials. We could also be precluded from billing third-party payers for tests for which the underlying informed consents are challenged, or we could be requested to refund amounts previously paid by third-party payers for such tests. We could become involved in legal challenges or regulatory enforcement, which could require significant management and financial resources and adversely affect our operating results.
Risks Related to Government Regulation
We may be adversely impacted by changes in laws and regulations, or in their application.
The health care industry in which we operate is highly regulated, and failure to comply with applicable regulatory, supervisory, accreditation, registration, or licensing requirements may adversely affect our business, operating results, and financial condition. The laws and regulations governing our research and marketing efforts are extremely complex and in many instances there are no clear regulatory or judicial interpretations of these laws and regulations, which increases the risk that we may be found to be in violation of these laws.
Furthermore, the industry is growing, and regulatory agencies such as HHS or the FDA may apply heightened scrutiny to new developments. While we have taken steps to ensure compliance with current regulatory frameworks in all material respects as historically enforced by the applicable regulatory agencies, given the highly complex and often unclear guidelines, there could be areas where we are unintentionally and unknowingly noncompliant. Any change in the federal or state laws or regulations relating to our business may require us to implement changes to our business or practices, and we may not be able to do so in a timely or cost-effective manner. Should we be found to be noncompliant with current or future regulatory requirements, we may be subject to sanctions that could include changes to our operations, adverse publicity, substantial financial penalties, exclusion from state and federal health care programs, and criminal proceedings, which may adversely affect our business, operating results, and financial condition by increasing our cost of compliance or limiting our ability to develop, market, and commercialize our products.
In addition, there has been a longstanding trend of heightened U.S. federal and state scrutiny of payments made to physicians and other referral sources, which are governed by various state and federal laws and regulations including the Stark Law, the federal Anti-Kickback Statute, the Physician Payments Sunshine Act, the Eliminating Kickbacks in Recovery Act of 2018, and the federal False Claims Act, as well as state equivalents of such laws.
While we have implemented and strive to continuously develop and improve compliance policies and procedures intended to address compliance with applicable federal and state laws and regulations, including applicable fraud and abuse laws and regulations such as those described in this risk factor, the evolving compliance environment and the need to build and maintain robust and scalable systems to comply with regulations in multiple jurisdictions with different compliance and reporting requirements increases the possibility that we could inadvertently violate one or more of these requirements.
Changes in the way the FDA regulates the reagents, other consumables, and testing equipment we use when developing, validating, and performing our tests could result in delay or additional expense in bringing our tests to market or performing such tests for our customers.
Many of the sequencing instruments, reagents, kits, and other consumable products used to perform our testing, as well as the instruments and other capital equipment that enable the testing, are offered for sale as analyte specific reagents, or ASRs, or for research use only, or RUO. ASRs are medical devices and must comply with FDA quality system requirements provisions and other device requirements, but most are exempt from premarket review by the FDA as an in vitro diagnostic product. Products that are intended for RUO and are labeled as RUO are exempt from compliance with most FDA requirements, including the approval or clearance and other product quality requirements for medical devices. A product labeled RUO but which is actually intended for clinical diagnostic use may be viewed by the FDA as adulterated and misbranded under the Federal Food, Drug and Cosmetic Act, or the FD&C Act, and subject to FDA enforcement action. The FDA has said that when determining the intended use of a product labeled RUO, it will consider the totality of the circumstances surrounding distribution and use of the product, including how the product is marketed and to whom. The FDA could disagree with a supplier’s assessment that the supplier’s products are RUOs, or could conclude that products labeled as RUO are actually intended for clinical diagnostic use, and could take enforcement action against the supplier, including requiring the supplier to cease offering the product while it seeks appropriate marketing authorization from FDA. Suppliers of ASRs and RUO products that we employ in our tests may cease selling their respective products, and we may be unable to obtain an acceptable substitute on commercially reasonable terms or at all, which could significantly and adversely affect our ability to provide timely testing results to our customers or could significantly increase our costs of conducting business.
If we fail to comply with federal and/or state laboratory licensing requirements, we could lose the ability to perform our tests or experience disruptions to our business.
As a clinical laboratory, our business is subject to regulation by CMS through its Clinical Laboratory Improvement Amendments of 1988, or CLIA, program. The CLIA program regulates the quality of most laboratory testing performed on human specimens in the United States. CLIA regulations establish quality standards for laboratory testing in an effort to ensure the accuracy, reliability, and timeliness of patient results. To that same end, CLIA regulations require clinical laboratories to obtain a CLIA certificate and to meet specific standards with respect to operations, personnel, facilities, quality control and assurance, administration, participation in proficiency testing, and patient test management. CLIA certification is also required in order for us to be eligible to bill federal and state health care programs, as well as commercial insurers for our tests. To renew and maintain our CLIA certification, we are subject to survey and inspection every two years. Our laboratory holds a CLIA Certificate of Accreditation.
Our laboratory is also accredited by the College of American Pathologists, or CAP. CMS has deemed CAP standards to be equally or more stringent than CLIA regulations and has approved CAP as a recognized accrediting organization. Inspection by CAP is performed in lieu of inspection by CMS for CAP-accredited laboratories. Because we are accredited by CAP, we are deemed to also comply with CLIA. Many commercial insurers require CAP accreditation as a condition to contracting with clinical laboratories to cover their tests.
In the event of any CLIA-related violations, CMS has the authority to impose a wide range of sanctions, including revocation of the CLIA certification, directed plans of correction, onsite monitoring, civil monetary penalties, civil injunctive suits, a bar on the ownership or operation of a CLIA-certified laboratory by any owners or operators of the deficient laboratory, and many others, depending on the nature of the CLIA violation. Any sanction imposed under CLIA and its implementing regulations, including but not limited to those applicable to proficiency testing, or our failure to renew a CLIA certificate, could have a material and adverse effect on our business, operating results and financial condition. If we were to lose our CLIA certification, we would not be able to operate our clinical laboratory or conduct our testing, which would adversely impact our business, operating results, and financial condition. In such case, even if we were able to bring our laboratory back into compliance, we could incur significant expenses and lose revenue while doing so. Failure to maintain CAP accreditation could likewise have a material adverse effect on the sales of our tests and the results of our operations.
Our laboratory is located in Salt Lake City, Utah. Utah requires that laboratories located in this state hold a CLIA certificate (which we do), as well as approval from the Utah Department of Health, or UT DOH, to operate a laboratory. In addition to meeting CLIA requirements and holding a valid CLIA certificate, Utah requires that our laboratory timely notify the UT DOH of certain changes and demonstrate successful performance of proficiency testing in an approved proficiency testing program or approved alternative testing program. If our clinical laboratory is out of compliance with these standards, the UT DOH may revoke our approval to perform testing or potentially impose other remedial measures, any of which could materially affect our business. We maintain an approval in good standing with the UT DOH.
Moreover, several states require that out-of-state laboratories hold laboratory licenses from those states in order to test specimens from patients, or accept specimens from laboratories, in those states. One such state is New York. As part of the laboratory licensure process, the New York Department of Health, or NY DOH, requires that laboratories seeking licensure establish the analytic and clinical performance characteristics of all tests performed, and also imposes specific review and approval requirements on certain categories of testing, including laboratory developed tests, or LDTs. As an LDT, our PreTRM test is thus subject to this NY DOH review and approval process.
We have obtained licenses from states where we believe we are required to be licensed. From time to time, we may become aware of other states that require out-of-state laboratories to obtain licensure in order to accept specimens from those states, and it is possible that other states do have such requirements or will have such requirements in the future. If we identify any other state with such requirements or if we are contacted by any other state advising us of such requirements, we expect to seek to comply with such requirements. However, there is no assurance that we will be able to obtain any such required license for the particular state.
If a clinical laboratory is out of compliance with state laboratory licensure laws and regulations, the state authority may suspend, restrict or revoke the license to operate the clinical laboratory, assess substantial civil money penalties, or impose specific corrective action plans. If we were to lose a required state license, we would not be able to operate our clinical laboratory and conduct our tests, in full or in particular states, which would adversely impact our business, operating results, and financial condition. Any such actions could materially affect our business.
The FDA may finalize its rulemaking to regulate Laboratory Developed Tests or Congress may take action to reform the current legal requirements applicable to LDTs. In either case we may become subject to extensive regulatory requirements and may be required to conduct additional clinical trials prior to continuing to sell our existing tests or launching any other tests we may develop, which may increase the cost of conducting, or otherwise harm, our business.
We currently market the PreTRM test as an LDT and may in the future market other tests as LDTs. Although historically the FDA applied a policy of enforcement discretion with respect to LDTs whereby the agency does not generally actively enforce its regulatory requirements for such tests, in October 2023, the FDA issued a proposed rule aimed at regulating LDTs under the current medical device framework and phasing out its current enforcement discretion policy over several years. This FDA rulemaking was initiated after years of failed congressional attempts to harmonize the regulatory paradigms applicable to LDTs and other in vitro diagnostic tests, as discussed further below. FDA’s proposal envisions that the LDT enforcement policy phase-out process would occur in gradual stages over a total period of four years, with premarket approval applications for high-risk tests to be submitted by the 3.5-year mark, although more details are expected to be provided with the upcoming final rule. The likelihood of the FDA finalizing its proposed rule in April 2024 (as currently projected), as well as potential litigation challenging its authority to take such action, is uncertain at this time. Affected stakeholders continue to press for a comprehensive legislative solution to create a harmonized paradigm for oversight of LDTs by both the FDA and CMS, instead of administrative agency action, which may be disruptive to the industry and to patient access to certain diagnostic tests. If there are changes in FDA regulations or legislative authorities such that the agency begins to exercise oversight over LDTs, or if the FDA disagrees that our marketed tests are within the scope of its criteria used for defining LDTs, we may become subject to extensive regulatory requirements and may be required to stop selling our existing test or launching any other tests we may develop and to conduct additional clinical trials or take other actions prior to continuing to market our tests. If the FDA allows our tests to remain on the market but there is uncertainty about our tests, if they are labeled investigational by the FDA or if labeling claims the FDA allows us to make are very limited, orders from health care providers or reimbursement for our tests may decline.
While we believe that we are currently in material compliance with applicable laws and regulations as historically enforced by the FDA with respect to LDTs, we cannot assure you that the FDA will agree with our determination. A determination that we have violated these laws and regulations, or a public announcement that we are being investigated for possible violations, could adversely affect our business, prospects, results of operations, and financial condition.
Moreover, if the FDA were to disagree with our conclusion that the PreTRM test falls within the scope of the agency’s LDT definition and that the PreTRM test is thus subject to FDA’s medical device authorities and implementing regulations today, even in the absence of final rulemaking to regulate all LDTs as devices, the agency could require that we obtain premarket approval or another type of device premarket authorization in order for us to commercialize the PreTRM test. As part of this process, we may also be required to conduct additional clinical testing before applying for commercial marketing authorization. Clinical trials must be conducted in compliance with FDA regulations in order to support a marketing submission to the agency for a regulated product, or the FDA may take certain enforcement actions or reject the data. Performing additional, new clinical studies and trials in order to obtain product approval from the FDA, if any were to become necessary, would take a significant amount of time and would substantially delay our ability to commercialize the PreTRM test, any or all of which would adversely impact our business. Any such clinical trial may need to comply with recent amendments to the FD&C Act requiring sponsors of most clinical studies of investigational devices to develop and submit a diversity action plan to the FDA. If we were to be required to develop a diversity action plan for any future clinical trial, such an obligation could result in further costs and potentially delay our ability to begin such a clinical trial.
In addition, as noted above, Congress has been working on legislation to create an LDT and In Vitro Diagnostic, or IVD, regulatory framework that would be separate and distinct from the existing medical device regulatory framework. For example, as drafted and re-introduced for consideration by the current Congress, reform legislation called the Verifying Accurate, Leading-edge IVCT Development (VALID) Act would codify the term “in vitro clinical test,” or IVCT, and create a new medical product category separate from medical devices to include products currently regulated as IVDs as well as LDTs, among other provisions. The VALID Act would also create a new system for laboratories to use to submit their tests electronically to the FDA for approval, which is aimed at reducing the amount of time it would take for the agency to approve such tests, and establish a new program to expedite the development of diagnostic tests that can be used to address a current unmet need for patients. The FDA’s October 2023 publication of an LDT proposed rule that would apply the existing medical device framework to laboratory-developed products has renewed stakeholder calls for a more targeted approach to modernizing the federal government’s oversight of clinical diagnostic tests. It remains possible that congressional action in this area could displace the need for the FDA to complete its recently proposed rulemaking.
If Congress were to pass the VALID Act or any other legislation applicable to the FDA’s regulation of LDTs, or if the FDA were to successfully promulgate new regulations for such products through the ongoing notice-and-comment rulemaking or a future rulemaking proceeding, we will likely be subject to increased regulatory burdens such as registration and listing requirements, adverse event reporting requirements, and quality control requirements. Any legislation or formal FDA regulatory framework affecting LDTs is also likely to have premarket application requirements prohibiting commercialization without FDA authorization and controls regarding modification to the tests that may require further FDA submissions. Any such process would likely be costly and time-consuming.
The outcome and ultimate impact on our business of any changes to the federal government’s regulation of LDTs is difficult to predict. Potential future increased regulation of our LDTs could result in increased costs and administrative and legal actions for noncompliance, including warning letters, fines, penalties, product suspensions, product recalls, injunctions and other civil and criminal sanctions, which could have a material and adverse effect upon our business, operating results, and financial condition.
Furthermore, should it be required in the future, we cannot be sure that the PreTRM test, any new tests that we may develop, or new uses for our products that we may develop, will be reviewed and authorized for marketing by the FDA in a timely or cost-effective manner, if authorized at all. Even if such tests are authorized for marketing by the FDA, the agency could limit the test’s indications for use, which may significantly limit the market for that product and may adversely affect our business and financial condition. In addition, failure to comply with any applicable FDA requirements could trigger a range of governmental enforcement actions, including but not limited to warning letters, civil monetary penalties, injunctions, criminal prosecution, recall or seizure, operating restrictions, partial suspension or total shutdown of operations and denial of or challenges to applications for marketing authorization, as well as significant adverse publicity.
If we were to be required by the FDA to conduct additional clinical studies before continuing to offer the PreTRM test or future tests that we may develop as LDTs, those studies could lead to delays or failure to obtain necessary regulatory authorization, which could cause significant delays in commercializing any future products and harm our ability to achieve profitability.
If the FDA decides to require that we obtain any form or type of premarket authorization in order for us to commercialize our current PreTRM test or any future tests developed as LDTs, whether as a result of new legislative authority or following finalization and implementation of the October 2023 proposed rule or based on its determination that
the PreTRM test does not meet the definition of an LDT, we may be required to conduct additional clinical testing before submitting a regulatory submission for commercial marketing authorization. Clinical trials to support marketing authorization from the FDA must be conducted in compliance with various regulatory requirements, including investigational device exemption regulations and good clinical practices, or else the FDA may take certain enforcement actions or reject the data. Such clinical trials may take several years to design and conduct, and they are often expensive and resource-driven.
Further, even if clinical trials are completed as planned, we cannot be certain that their results would be able to support the PreTRM test’s claims or that the FDA will agree with our conclusions regarding the results of our clinical trials. If we are required to conduct clinical trials to support a premarket submission to the FDA, whether using prospectively acquired samples or archival samples, delays in the commencement or completion of clinical testing could significantly increase the development costs for the PreTRM test or any future tests and delay commercialization. Many of the factors that may cause or lead to a delay in the commencement or completion of clinical trials may also ultimately lead to delay or denial of regulatory authorization. See related risks described above at “The results of our clinical trials and studies may not support the use of our tests and other product candidates, or may not be replicated in later studies.”
The Federal Trade Commission and/or state enforcement or regulatory agencies may object to the methods and materials we use to promote our tests and initiate enforcement against us, which could adversely affect our business and financial condition.
The Federal Trade Commission, or FTC, and/or state enforcement or regulatory agencies (including but not limited to the offices of state attorneys general) may object to the materials and methods we use to promote our current tests or other LDTs we may develop in the future, including with respect to the product claims in our promotional materials, and may initiate enforcement actions against us. Enforcement actions by the FTC may include, among others, injunctions, civil penalties, and equitable monetary relief. Recently the FTC has become more active in its scrutiny of health claims used in advertising goods and services, including through its publication of a sweeping “health products compliance guidance” document in December 2022.
Medical product manufacturers’ use of social media platforms presents new risks.
We believe that our customer base and potential patient populations are active on social media and we have begun engaging through those platforms to elevate our national marketing presence. Social media practices in the diagnostic, pharmaceutical, biotechnology, and medical device industries are evolving, which creates uncertainty and risk of noncompliance with regulations applicable to our business. For example, patients may use social media platforms to comment on the effectiveness of, or adverse experiences with, the PreTRM test or any future products we may develop, which could result in reporting obligations or the need for us to conduct an investigation. In addition, there is a risk of inappropriate disclosure of sensitive information or negative or inaccurate posts or comments about us or our testing products on any social networking website. If any of these events were to occur or we otherwise fail to comply with any applicable regulations, we could incur liability, face restrictive regulatory actions, or incur other harm to our business.
Actual or perceived failures to comply with applicable data protection, data privacy and information security laws, regulations, standards, and other requirements could adversely affect our business, results of operations, and financial condition.
The global data protection landscape is rapidly evolving, and we are or may become subject to numerous state and federal laws, requirements, and regulations governing the collection, use, disclosure, retention, and security of personal information. Implementation standards and enforcement practices are likely to remain uncertain for the foreseeable future, and we cannot yet determine the impact future laws, regulations, or standards or perception of their requirements may have on our business. This evolution may create uncertainty in our business, affect our ability to operate in certain jurisdictions or to collect, store, transfer, use and share personal information, necessitate the acceptance of more onerous obligations in our contracts, result in liability, or impose additional costs on us. The cost of compliance with these laws, regulations, and standards is high and is likely to increase in the future. Any failure or perceived failure by us to comply with federal or state laws or regulations, our internal policies and procedures, or our contracts governing our use and disclosures of personal information could result in negative publicity, government investigations and enforcement actions, claims by third parties, and damage to our reputation, any of which could have a material adverse effect on our operations, financial performance, and business.
As our operations and business grow, we may become subject to or affected by new or additional privacy and security laws and regulations and face increased scrutiny or attention from regulatory authorities. In the United States, HIPAA requires organizations like ours to develop and implement policies and procedures with respect to information that is protected under HIPAA, called protected health information, or PHI, that is used or disclosed in connection with our testing services, including the adoption of administrative, physical, and technical safeguards to protect such information.
HIPAA further requires organizations subject to HIPAA, called “covered entities” to notify affected individuals without unreasonable delay and in no case later than 60 calendar days following discovery, of certain unauthorized access, uses, or disclosures of PHI. If a breach affects 500 individuals or more in a particular state or jurisdiction, covered entities must report it to the HHS and local media contemporaneously with notice to affected individuals, and HHS will post information regarding the breach, including the name of the entity reporting the breach, on its public website. If a breach affects fewer than 500 individuals, the covered entity must notify HHS within the first 60 days of the following calendar year in which the breach occurred.
Penalties for failure to comply with HIPAA are substantial and could include corrective action plans, and/or the imposition of civil monetary or criminal penalties. HIPAA also authorizes state attorneys general to enforce HIPAA on behalf of state residents. Courts can award damages, costs, and attorneys’ fees related to violations of HIPAA in such cases. While HIPAA does not create a private right of action allowing individuals to sue us in civil court for HIPAA violations, its standards have been used as the basis for a duty of care claim in state civil suits such as those for negligence or recklessness in the misuse or breach of PHI.
Certain states have also adopted privacy and security laws and regulations, some of which may be more stringent than HIPAA and/or regulate information other than PHI. Such laws and regulations will be subject to interpretation by various courts and other governmental authorities, thus creating potentially complex compliance issues for us and our future customers and strategic partners. At the state level, for example, California has enacted the California Consumer Privacy Act, or CCPA, an extremely comprehensive and stringent privacy law. The CCPA took effect on January 1, 2020, and became enforceable by the California Attorney General on July 1, 2020. It creates individual privacy rights for California consumers and increases the privacy and security obligations of entities handling certain personal data. The CCPA provides for civil penalties for violations, as well as a private right of action for data breaches. CCPA does not apply to health information that is protected by HIPAA or the California Confidentiality of Medical Information Act, but CCPA still applies to other types of personal information held by HIPAA covered entities, such as personnel or marketing information. The regulations issued under the CCPA have been modified several times, and there is still some uncertainty about how the law will be interpreted and enforced.
In addition, California voters also approved a new privacy law, the California Privacy Rights Act, or CPRA, on November 3, 2020 which went into effect in January 2023 with enforcement commencing in July 2023. CPRA modifies the CCPA significantly, resulting in further uncertainty, additional costs and expenses stemming from efforts to comply, and additional potential for harm and liability for failure to comply. The CPRA imposes additional obligations on companies covered by the legislation and expands consumers’ rights with respect to certain sensitive personal information. The CPRA also creates a new state agency vested with authority to implement and enforce the CCPA and the CPRA. A number of other states have enacted their own privacy laws, including Colorado, Connecticut, Delaware, Florida, Indiana, Iowa, Montana, Oregon, Tennessee, Texas, Utah, and Virginia, increasing our regulatory compliance burden and risk. Similar laws have also been proposed in other states and at the federal level.
The CCPA, the CPRA, and similar laws may increase our compliance costs and potential liability. Any liability from failure to comply with the requirements of these laws could adversely affect our financial condition. All U.S. states have implemented data breach notification laws that overlap and often conflict with HIPAA and apply simultaneously. We must comply with all of these laws simultaneously in the event of a data breach which is a complicated and expensive proposition.
The regulatory framework governing the collection, storage, use, and sharing of certain information, particularly financial and other personal information, is rapidly evolving and is likely to continue to be subject to uncertainty and varying interpretations. It is possible that these laws may be interpreted and applied in a manner that is inconsistent with our existing practices. Any failure or perceived failure by us, or any third parties with which we do business, to comply with our privacy policies, changing expectations, evolving laws, rules and regulations, industry standards, or contractual obligations to which we or such third parties are or may become subject, may result in actions or other claims against us by governmental entities or private actors, the expenditure of substantial costs, time and other resources or the incurrence of significant fines, penalties or other liabilities. In addition, any such action, particularly to the extent we were found to be
guilty of violations or otherwise liable for damages, would damage our reputation and adversely affect our business, financial condition, and results of operations.
Although we strive to comply with applicable laws, regulations and standards, our contractual obligations, and other legal obligations, these requirements are evolving and may be modified, interpreted, and applied in an inconsistent manner from one jurisdiction to another, and may conflict with one another or other legal obligations with which we must comply. Any failure or perceived failure by us or our employees, representatives, contractors, consultants, Contract Research Organizations, or CROs, collaborators, or other third parties to comply with such requirements or adequately address privacy and security concerns, even if unfounded, could result in additional cost and liability to us, damage our reputation, and adversely affect our business and results of operations.
Security breaches, losses of data, and other disruptions could compromise sensitive information related to our business or prevent us from accessing critical information and expose us to liability, which could adversely affect our business and reputation.
In the ordinary course of our business, we collect and store sensitive data, including PHI (such as patient medical records, including test results), and personally identifiable information. We also store business and financial information, intellectual property, research and development information, trade secrets, and other proprietary and business critical information, including that of our customers, payers and collaboration partners. We manage and maintain our data utilizing a combination of on-site systems, managed data center systems and cloud-based data center systems. We are highly dependent on information technology networks and systems, including the internet, to securely process, transmit and store critical information. Although we take measures to protect sensitive information from unauthorized access or disclosure, our information technology and infrastructure, and that of our third-party billing and collections provider and other service providers, may be vulnerable to attacks by hackers, viruses, disruptions and breaches due to employee error or malfeasance.
A security breach or privacy violation that leads to unauthorized access, disclosure or modification of, or prevents access to, patient information, including PHI, could implicate state and federal breach notification laws, subject us to fines and mandatory corrective action and require us to verify the correctness of, or to reconstruct, database contents. Such a breach or violation also could result in legal claims or proceedings brought by a private party or a governmental authority, liability under laws and regulations that protect the privacy of personal information, such as HIPAA and laws and regulations of various U.S. states, as well as penalties imposed by the Payment Card Industry Security Standards Council for violations of the Payment Card Industry Data Security Standards. If we are unable to prevent such security breaches or privacy violations or implement satisfactory remedial measures, we may suffer loss of reputation, financial loss, and civil or criminal fines or other penalties. In addition, these breaches and other forms of inappropriate access can be difficult to detect, and any delay in identifying them may lead to increased harm of the type described above.
Unauthorized access, loss, or dissemination of information could disrupt our operations, including our ability to perform tests, provide test results, bill payers or patients, process claims and appeals, provide customer assistance services, conduct research and development activities, develop and commercialize tests, collect, process and prepare company financial information, provide information about our tests, educate patients and health care providers about our service, and manage the administrative aspects of our business, any of which could damage our reputation and adversely affect our business. Any breach could also result in the compromise of our trade secrets and other proprietary information, which could adversely affect our competitive position.
Any failure or perceived failure by us or any third-party collaborators, service providers, contractors or consultants to comply with privacy, confidentiality, data security or similar obligations, or any data security incidents or other security breaches that result in the accidental, unlawful or unauthorized access to, use of, release of, or transfer of sensitive information, including personally identifiable information, or PHI, may result in negative publicity, harm to our reputation, governmental investigations, enforcement actions, regulatory fines, litigation or public statements against us, could cause third parties to lose trust in us or could result in claims by third parties, including class action lawsuits, any of which could have a material adverse effect on our reputation, business, financial condition or results of operations. While we have implemented data security measures intended to protect our information, data, information technology systems, applications and infrastructure, there can be no assurance that such measures will successfully prevent service interruptions or data security incidents or that these measures will be satisfactory to regulatory authorities in the event of an audit, investigation or complaint.
If we, or our employees or contractors on our behalf, engage in conduct that violates health care laws, are suspected or accused of engaging in such conduct, or are subject to investigation for actual or alleged such conduct, we could face substantial penalties and damage to our reputation, and our business operations and financial condition could be adversely affected.
We operate in one of the most highly regulated industries in the United States. Our business activities are, or may in the future be, subject to comprehensive compliance obligations under state and federal laws and regulations, including:
•Federal and state laws governing laboratory testing, including but not limited to the Clinical Laboratory Improvement Amendments of 1988 and state laboratory licensure and related laws.
•FDA laws and regulations, including but not limited to requirements for offering LDTs.
•The federal Anti-Kickback Statute, or AKS, which generally prohibits, among other things knowingly and willfully offering, paying, soliciting, or receiving any remuneration, directly or indirectly, covertly or overtly, in cash or in kind in return for (i) referring an individual to a person for the furnishing or arranging of any item or service, or (ii) purchasing, leasing, ordering, or arranging for or recommending the purchasing, leasing, or ordering of any good, facility, service, or item, for which payment may be made by federal health care programs. A person or entity does not need to have actual knowledge of the AKS or specific intent to violate it to have committed a violation. Safe harbors and exceptions to the AKS protect specified arrangements and conduct if every element of the applicable safe harbor or exception is met. However, failure to satisfy each such requirement does not necessarily mean that the arrangement or conduct at issue violates the AKS. In such circumstances, a facts-and-circumstances analysis is necessary to determine AKS compliance or lack thereof. Violations of the AKS are subject to civil and criminal fines and penalties for each violation, plus up to three times the remuneration involved, imprisonment, and exclusion from federal health care programs. In addition, claims submitted to federal health care programs for items or services resulting from a violation of the AKS are deemed to be false or fraudulent claims for purposes of the False Claims Act, or FCA.
•The Stark Law, also known as the physician self-referral prohibition, which, unless an exception applies, generally prohibits physicians or an immediate family member from making referrals for certain designated health services covered by Medicare or Medicaid, including clinical laboratory services, if the physician or an immediate family member has a prohibited financial relationship with the entity providing the services at issue. Many states have statutes that are similar to the Stark Law. Federal and state enforcement agencies may assert that a claim including items or services resulting from a violation of the Stark Law or state law equivalent constitutes a false or fraudulent claim for purposes of the federal FCA or any state false claims statute.
•The federal False Claims Act imposes civil liability on any person or entity that, among other things, knowingly presents, or causes to be presented, to the federal government, claims for payment that are false or fraudulent; and/or knowingly makes, uses, or causes to be made or used, a false statement or record material to a false or fraudulent claim or obligation to pay or transmit money or property to the federal government. The FCA also prohibits the knowing retention of overpayments (sometimes referred to as “reverse false claims”) and permits private individuals acting as “whistleblowers” (also referred to as qui tam relators) to bring actions on behalf of the federal government alleging violations of the FCA and to share in any monetary recovery. The federal government may elect or decline to intervene in such matters, but if the government declines intervention, the whistleblower may still proceed with the litigation on the government’s behalf.
•The federal Civil Monetary Penalties Law, or CMP Law, which, unless an exception applies, prohibits, among other things, (1) the offering or transfer of remuneration to a beneficiary of Medicare or a state health care program, if the person knows or should know it is likely to influence the beneficiary’s selection of a particular provider, practitioner, or supplier of services reimbursable by Medicare or a state health care program; (2) employing or contracting with an individual or entity that the provider knows or should know is excluded from participation in a federal health care program; (3) billing for services requested by an unlicensed physician or an excluded provider; and (4) billing for medically unnecessary services. Violations of the CMP Law may result in the imposition of civil monetary penalties, as well as damages and possible exclusion from participation in state and federal health care programs.
•The federal health care fraud statute, which imposes criminal liability for knowingly and willfully executing or attempting to execute a scheme to defraud any health care benefit program (which includes commercial insurers). Violations of this statute are punishable by imprisonment, fines, or both.
•The federal statute prohibiting false statements relating to health care matters, which criminalizes knowingly and willfully falsifying, concealing or covering up by any trick or device a material fact or making any materially
false, fictitious, or fraudulent statements or representations in connection with the delivery of, or payment for, health care benefits, items or services relating to health care matters. Violations of this statute are punishable by imprisonment, fines, or both.
•HIPAA, as amended by HITECH and its respective implementing regulations, including the Final Omnibus Rule published in January 2013, which impose requirements on certain covered health care providers, health plans, and health care clearinghouses as well as their respective business associates. HITECH also created new tiers of civil monetary penalties, amended HIPAA to make civil and criminal penalties directly applicable to business associates, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce HIPAA and seek attorneys’ fees and costs associated with pursuing federal civil actions. There are additional federal, state, and non-U.S. laws which govern the privacy and security of health and other personal information, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts.
•The Eliminating Kickbacks in Recovery Act of 2018, or EKRA, which is an all-payer anti-kickback law that criminalizes the offer, payment, solicitation, or receipt of any remuneration, directly or indirectly, overtly or covertly, in cash or in kind, in return for referring, to induce referrals of, or in exchange for referring patients to recovery homes, clinical treatment facilities, or laboratories, unless an exception applies. Most of the safe harbors applicable under the AKS are not reiterated under EKRA’s exceptions. Therefore, compliance with an AKS safe harbor may not guarantee protection under the EKRA. EKRA thus could be interpreted to potentially expand the universe of arrangements that could be subject to enforcement under federal fraud and abuse laws, as well as substantial penalties.
•State data privacy and security laws, which may be more stringent than HIPAA. For example, the CCPA creates individual privacy rights for California consumers and increases the privacy and security obligations of certain entities handling certain personal data. The CCPA provides for civil penalties for violations, as well as a private right of action for data breaches. The CCPA is expected to increase data breach litigation and may increase our compliance costs and potential liability. Many similar laws have been proposed at the federal level and in other states; in the event that we are subject to or affected by any such privacy and data protection laws, any liability from failure to comply with the requirements of these laws could adversely affect our financial condition.
•Federal, state, and local regulations relating to the handling and disposal of regulated medical waste, hazardous waste, and biohazardous waste and workplace safety for health care employees.
•Laws and regulations relating to health and safety, labor and employment, public reporting, taxation, and other areas applicable to businesses generally, all of which are subject to change, including, for example, the significant changes to the taxation of business entities were enacted in December 2017.
•Additionally, we are subject to state equivalents of each of the health care laws and regulations described above, among others, some of which may be broader in scope and may apply regardless of the payer. Many U.S. states have adopted laws similar to the AKS, Stark Law, and FCA, which may apply to our business practices, including, but not limited to, research, distribution, sales or marketing arrangements, and claims involving health care items or services reimbursed by commercial insurers. In addition, many states have fraud and abuse laws, such as fee-splitting restrictions, insurance fraud laws, anti-markup laws, prohibitions on waiving coinsurance, copayments, deductibles and other amounts owed by patients, and prohibitions on the provision of tests at no or discounted cost to induce physician or patient adoption. Some states also prohibit certain health care practices, such as billing physicians for tests that they order and business corporations practicing medicine or employing or engaging physicians to practice medicine. There are ambiguities as to what is required to comply with these state requirements and if we fail to comply with an applicable state law requirement, we could be subject to penalties. Finally, there are state and foreign laws governing the privacy and security of health information, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
Because we develop our LDTs solely for use by or within our own laboratory, we believe we are exempt from the reporting requirements imposed under the federal Physician Payments Sunshine Act, or the Sunshine Act. The Sunshine Act requires, among other things, certain manufacturers of drugs, devices, biologics, and medical supplies reimbursed under Medicare, Medicaid or the Children’s Health Insurance Program to collect and report annually to CMS certain data and information related to payments and other transfers of value provided to physicians, teaching hospitals, and advanced non-physician health care practitioners, as well as ownership and investment interests, including such ownership and investment interests held by a physician’s immediate family members. A number of states also have laws similar to the Sunshine Act.
While we believe that the Sunshine Act does not apply to our business, we cannot guarantee that the federal government or other regulators will agree with our determination. Moreover, we could become subject to Sunshine Act reporting requirements if the FDA requires us to obtain premarket authorization for our tests as medical devices (whether because the agency determines that the PreTRM test does not fall within the scope of the agency’s existing LDT definition or because it finalizes the ongoing notice-and-comment rulemaking to exercise authority over LDTs as medical devices) or Congress enacts legislative reforms to the federal oversight of LDTs to subject them to FDA regulation and/or the reporting requirements of the Sunshine Act. A determination that we have violated these laws and related CMS regulations, or a public announcement that we are being investigated for possible violations, could adversely affect our business.
In addition, rapid growth and expansion of our business may increase the risk of violating applicable health care laws or related internal compliance policies and procedures, as well as the possibility that we may be accused of and/or investigated for violating these laws, regulations, and related internal policies and procedures. We likewise may be accused of, and subject to investigation and/or enforcement for, violating these laws on the basis of conduct engaged in by our employees, contractors and/or other related third parties. Such accusations and investigations may stem from allegations made by whistleblowers under the qui tam provisions of the FCA or state law equivalents, as well as investigative efforts undertaken by state and federal regulatory and enforcement agencies. The evolving interpretations of these laws and regulations by courts and regulators increase the risk that we may be alleged to be, or in fact found to be, in violation of these or other laws and regulations.
Because of the breadth of these laws and the narrowness of the statutory exceptions and safe harbors available, it is possible that some of our business activities could be subject to challenge and may not comply under one or more of such laws, regulations, and guidance. Law enforcement authorities are increasingly focused on enforcing fraud and abuse laws, and it is possible that some of our practices may be challenged under these laws. Efforts to ensure that our current and future business arrangements with third parties, and our business generally, will comply with applicable health care laws and regulations will involve substantial costs. If our operations, including our arrangements with physicians and other health care providers, are found to be in violation of any of such laws or any other governmental regulations that apply to us, we may be subject to penalties, including, without limitation, administrative, civil and criminal penalties, damages, fines, disgorgement, contractual damages, reputational harm, diminished profits and future earnings, the curtailment or restructuring of our operations, exclusion from participation in federal and state health care programs (such as Medicare and Medicaid), and imprisonment, as well as additional reporting obligations and oversight if we become subject to a corporate integrity agreement or other agreement to resolve allegations of non-compliance with these laws, any of which could adversely affect our ability to operate our business and our financial results.
Companies in our industry occasionally receive investigative demands, subpoenas, or other requests for information from state and federal governmental agencies. We cannot predict the occurrence, timing, outcome, or impact of any such investigations. Any adverse outcome in one or more of these investigations could include the commencement of civil and/or criminal proceedings, substantial fines, penalties, administrative remedies and/or entry into corporate integrity agreements with governmental agencies, among other penalties. In addition, resolution of any of these matters could involve the imposition of additional costly compliance obligations. These potential consequences, as well as any adverse outcome from government investigations, could have a material and adverse effect on our business, operating results, and financial condition.
Risks Related to Intellectual Property
Any failure to obtain, maintain, and enforce our intellectual property rights could impair our ability to protect our proprietary technology and our brand.
Our success and ability to compete depend, in part, on our ability to obtain, maintain, and enforce patents, trade secrets, trademarks, and other intellectual property rights and to operate without having third parties infringe, misappropriate, or circumvent the rights that we own or license. If we are unable to obtain, maintain, and enforce intellectual property protection covering our current and future tests or technology, others may be able to make, use or sell tests or technology that are substantially the same as ours without incurring the sizeable development costs that we have incurred, which would adversely affect our ability to compete in the market. Our ability to stop third parties from making, using, selling, offering to sell or importing our tests or technology is dependent upon the extent to which we have rights under valid and enforceable patents that cover these activities. However, the patent positions of diagnostic companies, including ours, can be highly uncertain and involve complex legal and factual questions for which important legal principles remain unresolved. The U.S. Supreme Court and U.S. Court of Appeals for the Federal Circuit have in recent years issued a number of decisions relating to the patent-eligibility of diagnostic method claims. We cannot predict what
impact these decisions may have on our ability to obtain or enforce patents relating to diagnostic methods in the future. We believe that no consistent policy regarding the scope of valid patent claims in these fields has emerged to date in the United States. The patent situation in the diagnostics industry outside the United States also is uncertain at least in a number of countries. Moreover, U.S. patent laws frequently change, including changes regarding how patent laws are interpreted, and the U.S. Patent and Trademark Office, or USPTO, frequently issues new procedures to the patent system. We cannot accurately predict future changes in the interpretation of patent laws or changes to patent laws that might be enacted into law. Those changes may materially affect our patents or our ability to obtain patents. Therefore, there can be no assurance that any current or future patent applications will result in the issuance of patents or that we will develop additional proprietary tests or technology which are patentable. Moreover, patents or pending applications that may issue in the future may not provide us with any competitive advantage. Our patent position is subject to numerous additional risks, including the following:
•we may fail to seek patent protection for inventions that are important to our success;
•any current or future patent applications may not result in issued patents;
•we cannot be certain that we were the first to file patent applications for the inventions covered by pending patent applications and, if we are not, we may be subject to priority or derivation disputes;
•we may be required to disclaim part or all of the term of certain patents or part or all of the term of certain patent applications;
•we may file patent applications but have claims restricted or we may not be able to supply sufficient data to support our claims and, as a result, may not obtain the original claims desired or we may receive restricted claims. Alternatively, it is possible that we may not receive any patent protection from an application;
•we could inadvertently abandon a patent or patent application, resulting in the loss of protection of certain intellectual property rights in a particular country. We or our patent counsel may take action resulting in a patent or patent application becoming abandoned which may not be able to be reinstated or if reinstated, may suffer patent term adjustments;
•the claims of our issued patents or patent applications when issued may not cover our tests or technology;
•no assurance can be given that our patents would be declared by a court to be valid and enforceable or that a competitor’s test or technology would be found by a court to infringe our patents. Our patents or patent applications may be challenged by third parties in patent litigation or in proceedings before the USPTO or its foreign counterparts, and may ultimately be declared invalid or unenforceable, or narrowed in scope;
•there may be prior art of which we are not aware that may affect the validity of a patent claim. There also may be prior art of which we are aware, but which we do not believe affects the validity or enforceability of a claim, which may, nonetheless, ultimately be found to do so;
•third parties may develop tests or technology that have the same or similar effect as our tests and technology without infringing our patents. Such third parties may also intentionally circumvent our patents by means of alternate designs or processes or file applications or be granted patents that would block or hurt our efforts;
•there may be patents relevant to our tests or technology of which we are not aware;
•certain of our intellectual property was partly supported by a U.S. government grant awarded by the National Institutes of Health, and the government accordingly has certain rights in this intellectual property, including a non-exclusive, non-transferable, irrevocable worldwide license to use applicable inventions for any governmental purpose. Such rights also include “march-in” rights, which refer to the right of the U.S. government to require us to grant a license to the technology to a responsible applicant if we fail to achieve practical application of the technology or if action is necessary to alleviate health or safety needs, to meet requirements of federal regulations or to give preference to U.S. industry;
•our patent counsel, lawyers or advisors may have given us, or may in the future give us incorrect advice or counsel;
•the patent and patent enforcement laws of some foreign jurisdictions may not protect intellectual property rights to the same extent as laws in the United States, and many companies have encountered significant difficulties in protecting and defending such rights in foreign jurisdictions. If we encounter such difficulties or we are otherwise precluded from effectively protecting our intellectual property rights in foreign jurisdictions, our business prospects could be substantially harmed, and we may not pursue or obtain patent protection in all major markets; and
•we may not develop additional tests or technology that are patentable.
Any of these factors could hurt our ability to gain patent protection for our tests and technology.
Issued patents covering our tests and technology could be found invalid or unenforceable, if challenged.
Our patents and patent applications may be subject to validity, enforceability and priority disputes. The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability. Some of our patents or patent applications may be challenged at a future point in time in opposition, derivation, reexamination, inter partes review, post-grant review or interference or other similar proceedings. Any successful third-party challenge to our patents in this or any other proceeding could result in the unenforceability or invalidity of such patents, which may lead to increased competition to our business, which could have a material adverse effect on our business, financial condition, results of operations, and prospects. In addition, if we initiate legal proceedings against a third party to enforce a patent covering our tests or technology, the defendant could counterclaim that such patent covering our tests or technology, as applicable, is invalid and/or unenforceable. In patent litigation in the United States, defendant counterclaims alleging invalidity or unenforceability are commonplace. There are numerous grounds upon which a third party can assert invalidity or unenforceability of a patent. Grounds for a validity challenge could be an alleged failure to meet any of several statutory requirements, including lack of novelty, obviousness or non-enablement. Grounds for an unenforceability assertion could be an allegation that someone connected with prosecution of the patent withheld relevant information from the relevant patent office, or made a misleading statement, during prosecution. Third parties may also raise similar claims before administrative bodies in the United States or abroad, even outside the context of litigation. Such mechanisms include ex parte re-examination, inter partes review, post-grant review, derivation and equivalent proceedings in non-U.S. jurisdictions, such as opposition proceedings. Such proceedings could result in revocation of or amendment to our patents in such a way that they no longer cover and protect our tests or technology. With respect to the validity of our patents, for example, we cannot be certain that there is no invalidating prior art of which we, our licensor, our or its patent counsel and the patent examiner were unaware during prosecution. The outcome following legal assertions of invalidity and unenforceability during patent litigation is unpredictable. If a defendant or other third party were to prevail on a legal assertion of invalidity or unenforceability, we would lose at least part, and perhaps all, of the patent protection on certain aspects of our tests and technology, which could have a material adverse effect on our business, financial condition, results of operations, and prospects. In addition, if the breadth or strength of protection provided by our patents and patent applications is threatened, regardless of the outcome, it could dissuade companies from collaborating with us to license intellectual property or develop or commercialize current or future tests and technology.
We may not be aware of all third-party intellectual property rights potentially relating to our tests or technology. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the United States and other jurisdictions are typically not published until approximately 18 months after filing or, in some cases, not until such patent applications issue as patents. We might not have been the first to make the inventions covered by each of our pending patent applications and we might not have been the first to file patent applications for these inventions. To determine the priority of these inventions, we may have to participate in interference proceedings, derivation proceedings or other post-grant proceedings declared by the USPTO, or other similar proceedings in non-U.S. jurisdictions, that could result in substantial cost to us and the loss of valuable patent protection. The outcome of such proceedings is uncertain. No assurance can be given that other patent applications will not have priority over our patent applications. In addition, changes to the patent laws of the United States allow for various post-grant opposition proceedings that have not been extensively tested, and their outcome is therefore uncertain. Furthermore, if third parties bring these proceedings against our patents, regardless of the merit of such proceedings and regardless of whether we are successful, we could experience significant costs and our management may be distracted. Any of the foregoing events could have a material adverse effect on our business, financial condition, results of operations, and prospects.
Our intellectual property may be infringed by a third party.
Third parties may infringe one or more of our patents, trademarks or other intellectual property rights. We cannot predict if, when or where a third party may infringe our intellectual property rights. To counter infringement, we may be required to file infringement lawsuits, which can be expensive and time consuming. There is no assurance that we would be successful in a court of law in proving that a third party is infringing one or more of our issued patents or trademarks. Any claims we assert against perceived infringers could also provoke these parties to assert counterclaims against us, alleging that we infringe their intellectual property. In addition, in a patent infringement proceeding, a court may decide that a patent of ours is invalid or unenforceable, in whole or in part, construe the patent’s claims narrowly and/or refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question,
any of which may adversely affect our business. Even if we are successful in proving in a court of law that a third party is infringing our intellectual property rights, there can be no assurance that we would be successful in halting their infringing activities, for example, through a permanent injunction, or that we would be fully or even partially financially compensated for any harm to our business. We may be forced to enter into a license or other agreement with the infringing third party at terms less profitable or otherwise commercially acceptable to us than if the license or agreement were negotiated under conditions between those of a willing licensee and a willing licensor. We may not become aware of a third-party infringer within legal timeframes for compensation or at all, thereby possibly losing the ability to be compensated for any harm to our business. Such a third party may be operating in a foreign country where the infringer is difficult to locate and/or the intellectual property laws may be more difficult to enforce. Some third-party infringers may be able to sustain the costs of complex infringement litigation more effectively than we can because they have substantially greater resources. Any inability to stop third-party infringement could result in loss in market share of some of our tests and technology or even lead to a delay, reduction and/or inhibition of the development, manufacture or sale of certain tests and technology by us. There is no assurance that a test or technology produced and sold by a third-party infringer would meet our or other regulatory standards or would be safe for use. Such third-party infringer tests or technology could irreparably harm the reputation of our tests or technology thereby resulting in substantial loss in our market share and profits.
Developments or uncertainty in the patent statute, patent case law or USPTO rules and regulations may impact the validity of our patent rights.
Our patent rights may be affected by developments or uncertainty in the patent statute, patent case law or USPTO rules and regulations. For example, the patent position of companies engaged in the development and commercialization of diagnostic tests are particularly uncertain. Changes in either the patent laws or interpretation of the patent laws in the United States or in other jurisdictions could increase the uncertainties and costs surrounding the prosecution of patent applications and the enforcement or defense of issued patents. For instance, under the Leahy-Smith America Invents Act, or the America Invents Act, enacted in September 2011, the United States transitioned to a first inventor to file system in which, assuming that other requirements for patentability are met, the first inventor to file a patent application is entitled to the patent on an invention regardless of whether a third party was the first to invent the claimed invention. These changes include allowing third-party submission of prior art to the USPTO during patent prosecution and additional procedures to challenge the validity of a patent by USPTO administered post-grant proceedings, including post-grant review, inter partes review and derivation proceedings. The America Invents Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents, all of which could have a material adverse effect on our business, financial condition, results of operations, and prospects.
Various courts, including the U.S. Supreme Court, have rendered decisions that impact the scope of patentability of certain inventions or discoveries relating to the life sciences technology. Specifically, these decisions stand for the proposition that patent claims that recite laws of nature are not themselves patentable unless those patent claims have sufficient additional features that provide practical assurance that the processes are genuine inventive applications of those laws rather than patent drafting efforts designed to monopolize the law of nature itself. What constitutes a “sufficient” additional feature is uncertain. Furthermore, in view of these decisions, since December 2014, the USPTO has published and continues to publish revised guidelines for patent examiners to apply when examining process claims for patent eligibility.
In addition, U.S. Supreme Court rulings have narrowed the scope of patent protection available in certain circumstances and weakened the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained. Depending on decisions by the U.S. Congress, the federal courts and the USPTO, the laws and regulations governing patents could change in unpredictable ways that may have a material adverse effect on our ability to obtain new patents and to defend and enforce our existing patents and patents that we might obtain in the future.
We cannot assure you that our patent portfolio will not be negatively impacted by the current uncertain state of the law, new court rulings or changes in guidance or procedures issued by the USPTO or other similar patent offices around the world. From time to time, the U.S. Supreme Court, other federal courts, the U.S. Congress or the USPTO may change the standards of patentability, scope and validity of patents within the life sciences technology and any such changes, or any similar adverse changes in the patent laws of other jurisdictions, could have a negative impact on our business, financial condition, prospects, and results of operations.
We may be subject to claims challenging the inventorship of our patents and other intellectual property.
We may be subject to claims that former employees, collaborators or other third parties have an interest in our patents, trade secrets or other intellectual property as an inventor or co-inventor. For example, we may have inventorship disputes arise from conflicting obligations of employees, consultants or others who are involved in developing our tests and technology. In addition, counterparties to our consulting, sponsored research, software development and other agreements may assert that they have an ownership interest in intellectual property developed under such arrangements. In particular, certain software development agreements pursuant to which certain third parties have developed parts of our proprietary software may not include provisions that expressly assign to us ownership of all intellectual property developed for us by such third parties. As such, we may not have the right to use all such developed intellectual property under such agreements, we may be required to obtain licenses from third parties and such licenses may not be available on commercially reasonable terms or at all, or may be non-exclusive. If we are unable to obtain such licenses and such licenses are necessary for the development, manufacture, and commercialization of our tests and technology, we may need to cease the development, manufacture, and commercialization of our tests and technology. Litigation may be necessary to defend against these and other claims challenging inventorship of our patents, trade secrets or other intellectual property. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, intellectual property that is important to our business, including our software, workflows, consumables, and reagent kits. In such an event, we may be required to obtain licenses from third parties and such licenses may not be available on commercially reasonable terms or at all, or may be non-exclusive. If we are unable to obtain and maintain such licenses, we may need to cease the development, manufacture, and commercialization of our tests and technology. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees, and certain customers or partners may defer engaging with us until the particular dispute is resolved. Any of the foregoing could have a material adverse effect on our business, financial condition, results of operations, and prospects.
We may be subject to claims that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of third parties.
We employ individuals who were previously employed at other biotechnology or diagnostic companies. We may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise used or disclosed confidential information of our employees’ former employers or other third parties. We may also be subject to claims that former employers or other third parties have an ownership interest in our patents. Litigation may be necessary to defend against these claims. There is no guarantee of success in defending these claims, and if we do not prevail, we could be required to pay substantial damages and could lose rights to important intellectual property. Even if we are successful, litigation could result in substantial cost and be a distraction to our management and other employees.
If we are not able to prevent disclosure of our trade secrets and other proprietary information, the value of our tests and technology could be significantly diminished.
We rely on trade secret protection to protect our interests in proprietary know-how and in processes for which patents are difficult to obtain or enforce, including the proprietary algorithm that we use for our tests and technology, including the PreTRM test. We may not be able to protect our trade secrets adequately. We have a policy of requiring our consultants, advisors, and collaborators to enter into confidentiality agreements and our employees to enter into invention, non-disclosure, and non-compete agreements. However, no assurance can be given that we have entered into appropriate agreements with all parties that have had access to our trade secrets, know-how or other proprietary information. There is also no assurance that such agreements will provide for a meaningful protection of our trade secrets, know-how or other proprietary information in the event of any unauthorized use or disclosure of information. Furthermore, we cannot provide assurance that any of our employees, consultants, contract personnel or collaborators, either accidentally or through willful misconduct, will not cause serious damage to our programs and our strategy, for example by disclosing important trade secrets, know-how or proprietary information to our competitors.
It is also possible that our trade secrets, know-how or other proprietary information could be obtained by third parties as a result of breaches of our physical or electronic security systems. Any disclosure of confidential data into the public domain or to third parties could allow our competitors to learn our trade secrets and use the information in competition against us. In addition, others may independently discover our trade secrets and proprietary information. Any action to enforce our rights is likely to be time consuming and expensive, and may ultimately be unsuccessful, or may result in a remedy that is not commercially valuable. These risks are accentuated in foreign countries where laws or law enforcement
practices may not protect proprietary rights as fully as in the United States or Europe. Any unauthorized disclosure of our trade secrets or proprietary information could harm our competitive position.
Risks Related to Our Class A Common Stock
The price of our Class A common stock may be volatile, and you could lose all or part of your investment.
The trading price of our Class A common stock is likely to be highly volatile and could be subject to wide fluctuations in response to various factors, some of which are beyond our control, including limited trading volume. In addition to the factors discussed in this “Risk Factors” section and elsewhere in this report, these factors include:
•our ability to successfully execute under our commercial agreement with Elevance Health and obtain broader market adoption of our PreTRM test;
•actual or anticipated variations in our and our competitors’ results of operations, as well as how those results compare to analyst and investor expectations;
•our failure to successfully commercialize our product candidates;
•announcements by us or our competitors of new products, significant acquisitions, other strategic transactions, including strategic and commercial partnerships and relationships, joint ventures, divestitures, collaborations or capital commitments;
•changes in reimbursement practices by current or potential payers;
•failure of analysts to initiate or maintain coverage of our Company, issuance of new securities analysts’ reports or changed recommendations for our Class A common stock;
•forward-looking statements related to our financial guidance or projections, our failure to meet or exceed our financial guidance or projections or changes in our financial guidance or projections;
•actual or anticipated changes in regulatory oversight of our products;
•development of disputes concerning our intellectual property or other proprietary rights;
•commencement of, or our involvement in, litigation;
•announcement or expectation of additional debt or equity financing efforts;
•any major change in our management;
•our inability to establish collaborations, if needed;
•additions or departures of key scientific or management personnel;
•our ability to effectively manage our growth;
•overall performance of the equity markets;
•sales of our common stock by us, our directors and officers, or our other stockholders in the future;
•trading volume of our Class A common stock;
•changes in accounting practices;
•ineffectiveness of our internal controls;
•general political and economic conditions; and
•other events or factors, many of which are beyond our control.
In addition, the stock market in general, and the market for diagnostics companies in particular, has experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of the companies, including as a result of inflationary pressures, supply chain disruptions and geopolitical instability. Broad market and industry factors may negatively affect the market price of our Class A common stock, regardless of our actual operating performance. In the past, securities class action litigation has often been instituted against companies following periods of volatility in the market price of a company’s securities. This type of litigation, if instituted, could result in substantial costs and a diversion of management’s attention and resources.
We do not intend to pay dividends on our Class A common stock, so any returns will be limited to the value of our Class A common stock.
We currently anticipate that we will retain future earnings for the development, operation and expansion of our business and do not anticipate declaring or paying any cash dividends for the foreseeable future. Furthermore, future debt or other financing arrangements may contain terms prohibiting or limiting the amount of dividends that may be declared or paid on our Class A common stock. Any return to stockholders will therefore be limited to the appreciation of their stock.
Our executive officers, directors and their affiliates and our stockholders holding 5% or more of our common stock own a significant percentage of our Class A common stock and will be able to exert significant control over matters subject to stockholder approval.
Our executive officers, directors and our stockholders holding 5% or more of our common stock and their affiliates beneficially hold a significant percentage of our outstanding Class A common stock. These stockholders, acting together, would be able to significantly influence our management and affairs and the outcome of matters submitted to our stockholders for approval, including the election of directors and any sale, merger, consolidation, or sale of all or substantially all of our assets. This concentration of ownership control may adversely affect the market price of our Class A common stock by:
•delaying, deferring or preventing a change in control;
•entrenching our management and the board of directors;
•impeding a merger, consolidation, takeover or other business combination involving us that other stockholders may desire; and/or
•discouraging a potential acquirer from making a tender offer or otherwise attempting to obtain control of us.
The dual class structure of our common stock may limit your ability to influence corporate matters and may limit your visibility with respect to certain transactions.
The dual class structure of our common stock may limit your ability to influence corporate matters. Holders of our Class A common stock are entitled to one vote per share, while holders of our Class B common stock are not entitled to any votes per share. Nonetheless, each share of our Class B common stock may be converted at any time into one share of our Class A common stock at the option of its holder by providing written notice to us, subject to the limitations provided for in our amended and restated certificate of incorporation. Consequently, if holders of our Class B common stock exercise their option to make this conversion, this will have the effect of increasing the relative voting power of those prior holders of our Class B common stock, and correspondingly decreasing the voting power of the holders of our Class A common stock, which may limit your ability to influence corporate matters. Additionally, stockholders who hold, in the aggregate, more than 10% of our Class A common stock and Class B common stock, but 10% or less of our Class A common stock, and are not otherwise an insider, may not be required to report changes in their ownership due to transactions in our Class B common stock pursuant to Section 16(a) of the Exchange Act, and may not be subject to the short-swing profit provisions of Section 16(b) of the Exchange Act.
We are an emerging growth company and a smaller reporting company, and we cannot be certain if the reduced reporting requirements applicable to emerging growth companies will make our Class A common stock less attractive to investors.
We are an emerging growth company, or EGC, as defined in the JOBS Act. For as long as we continue to be an EGC, we may take advantage of exemptions from various reporting requirements that are applicable to other public companies that are not EGCs, including not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act, reduced disclosure obligations regarding executive compensation in this report and our periodic reports and proxy statements and exemptions from the requirements of holding nonbinding advisory votes on executive compensation and stockholder approval of any golden parachute payments not previously approved. We may remain an EGC until the earliest to occur of: (1) the last day of the fiscal year in which we have at least $1.235 billion in annual revenue; (2) the last day of the fiscal year in which we are deemed to be a “large accelerated filer,” as defined in Rule 12b-2 under the Exchange Act, which would occur if the market value of our common stock held by non-affiliates exceeded $700.0 million as of the last business day of the second fiscal quarter of such year; (3) the date on which we have issued more than $1.0 billion in non-convertible debt securities during the prior three-year period; and (4) December 31, 2026.
We are also a smaller reporting company, meaning that the market value of our Class A common stock held by non-affiliates is less than $700.0 million and our annual revenue is less than $100.0 million during the most recently completed fiscal year. We may continue to be a smaller reporting company if either (1) the market value of our Class A common stock held by non-affiliates is less than $250.0 million or (2) our annual revenue is less than $100.0 million during the most recently completed fiscal year and the market value of our Class A common stock held by non-affiliates is less than $700.0 million. If we are a smaller reporting company at the time we cease to be an EGC we may continue to rely on exemptions from certain disclosure requirements that are available to smaller reporting companies. Specifically, as a smaller reporting company, we may choose to present only the two most recent fiscal years of audited financial statements in our Annual Report on Form 10-K and, similar to emerging growth companies, smaller reporting companies have reduced disclosure obligations regarding executive compensation.
We may choose to take advantage of some, but not all, of the available exemptions. We have taken advantage of reduced reporting burdens in this report. In particular, we have not included all of the executive compensation information that would be required if we were not an EGC. We cannot predict whether investors will find our Class A common stock less attractive if we rely on certain or all of these exemptions. If some investors find our Class A common stock less attractive as a result, there may be a less active trading market for our Class A common stock and our stock price may be more volatile.
Under the JOBS Act, EGCs can also delay adopting new or revised accounting standards until such time as those standards apply to private companies, which may make our financial statements less comparable to companies that comply with new or revised accounting pronouncements as of public company effective dates.
Sales of a substantial number of shares of our Class A common stock by our existing stockholders in the public market could cause our stock price to decline.
Substantially all of our shares of Class A common stock and Class B common stock are eligible for public sale, if they are registered under the Securities Act of 1933, as amended, or the Securities Act, or if they qualify for an exemption from registration under the Securities Act, including under Rules 144 or 701. If our existing stockholders sell, or indicate an intention to sell, substantial amounts of our Class A common stock in the public market, the trading price of our Class A common stock could decline.
Certain holders of shares of our common stock will be entitled to rights with respect to the registration of their shares under the Securities Act as provided under the terms of an investors’ rights agreement between us and the holders of our stock. Registration of these shares under the Securities Act would result in the shares becoming freely tradable without restriction under the Securities Act, except for shares held by affiliates, as defined in Rule 144 under the Securities Act. Any sales of securities by these stockholders could have a material adverse effect on the trading price of our common stock.
We have registered on Form S-8 all shares of common stock that are issuable under our existing equity compensation plan, including the 2011 Employee, Director and Consultant Equity Incentive Plan, as amended, or the 2011 Plan, which expired in 2021, the 2021 Equity Incentive Plan, or the 2021 Plan, and the 2021 Employee Stock Purchase Plan, or the 2021 ESPP, as well as the shares of common stock underlying option awards outstanding under the 2011 Plan. Additionally, the number of shares of our Class A common stock reserved for issuance under our 2021 Equity Plan automatically increases on January 1 of each year, beginning on January 1, 2022, by 4% of the total number of shares of our capital stock outstanding on December 31 of the preceding calendar year, or a lesser number of shares determined by our board of directors or compensation committee. Furthermore, the number of shares of our Class A common stock reserved for issuance under our 2021 ESPP automatically increases on January 1 of each year, beginning on January 1, 2022, by 1% of the total number of shares of our capital stock outstanding on December 31 of the preceding calendar year, or a lesser number of shares determined by our board of directors or compensation committee. Unless our board of directors elects not to increase the number of shares available for future grant each year, our stockholders may experience additional dilution. As a consequence, these shares can be freely sold in the public market upon issuance, subject to volume limitations applicable to affiliates.
Anti-takeover provisions under our charter documents and Delaware law could delay or prevent a change in control which could limit the market price of our Class A common stock and may prevent or frustrate attempts by our stockholders to replace or remove our current management.
Our amended and restated certificate of incorporation and amended and restated bylaws contain provisions that could delay or prevent a change in control of our Company or changes in our board of directors that our stockholders might consider favorable. Some of these provisions include:
•a board of directors divided into three classes serving staggered three-year terms, such that not all members of the board will be elected at one time;
•a prohibition on stockholder action through written consent, which requires that all stockholder actions be taken at a meeting of our stockholders;
•a requirement that special meetings of stockholders be called only by the board of directors acting pursuant to a resolution approved by the affirmative vote of a majority of the directors then in office;
•advance notice requirements for stockholder proposals and nominations for election to our board of directors;
•a requirement that no member of our board of directors may be removed from office by our stockholders except for cause and, in addition to any other vote required by law, upon the approval of not less than two-thirds of all outstanding shares of our voting stock then entitled to vote in the election of directors;
•a requirement of approval of not less than two-thirds of all outstanding shares of our voting stock to amend any bylaws by stockholder action or to amend specific provisions of our certificate of incorporation; and
•the authority of the board of directors to issue convertible preferred stock on terms determined by the board of directors without stockholder approval and which convertible preferred stock may include rights superior to the rights of the holders of common stock.
In addition, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the General Corporation Law of the State of Delaware, which may prohibit certain business combinations with stockholders owning 15% or more of our outstanding voting stock. These anti-takeover provisions and other provisions in our amended and restated certificate of incorporation and amended and restated bylaws could make it more difficult for stockholders or potential acquirers to obtain control of our board of directors or initiate actions that are opposed by the then-current board of directors and could also delay or impede a merger, tender offer or proxy contest involving our Company. These provisions could also discourage proxy contests and make it more difficult for you and other stockholders to elect directors of your choosing or cause us to take other corporate actions you desire. Any delay or prevention of a change in control transaction or changes in our board of directors could cause the market price of our Class A common stock to decline.
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about our business, our stock price and trading volume could decline.
The trading market for our Class A common stock will depend in part on the research and reports that securities or industry analysts publish about us or our business. We do not have any control over these analysts. If few analysts commence coverage of us, the trading of our stock would likely decrease. Even if we do obtain sufficient analyst coverage, there can be no assurance that analysts will provide favorable coverage. If one or more of the analysts who covers us downgrades our stock or publishes inaccurate or unfavorable research about our business, our stock price may decline. If one or more of these analysts ceases coverage of our Company or fails to publish reports on us regularly, demand for our stock could decrease, which might cause our stock price and trading volume to decline.
Our amended and restated certificate of incorporation designates certain courts as the sole and exclusive forum for certain types of actions and proceedings that may be initiated by our stockholders, which could limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us or our directors, officers, or employees.
Our amended and restated certificate of incorporation provides that, unless we consent in writing to an alternative forum, the Court of Chancery of the State of Delaware will be the sole and exclusive forum for any state law claims for (i) any derivative action or proceeding brought on our behalf, (ii) any action or proceeding asserting a claim of breach of fiduciary duty owed by any of our current or former directors, officers and employees, to us or our stockholders, (iii) any action or proceeding asserting a claim arising pursuant to any provision of the General Corporation Law of the State of Delaware, our amended and restated certificate of incorporation or our bylaws (in each case, as they may be amended from time to time), (iv) any action or proceeding to interpret, apply, enforce or determine the validity of our amended and
restated certificate of incorporation or bylaws, (v) any action or proceeding as to which the Delaware General Corporation Law confers jurisdiction to the Court of Chancery of the State of Delaware, or (vi) any action asserting a claim against us or any of our directors, officers or employees that is governed by the internal affairs doctrine; provided, however, that this exclusive forum provision will not apply to any causes of action arising under the Exchange Act. Our amended and restated certificate of incorporation will further provide that, unless we consent in writing to an alternative forum, the United States District Court for the District of Utah will be the exclusive forum for resolving any complaint asserting a cause of action arising under the Securities Act. We have chosen the United States District Court for the District of Utah as the exclusive forum for such Securities Act causes of action because our principal executive offices are located in Salt Lake City, Utah. In addition, our amended and restated certificate of incorporation will provide that any person or entity purchasing or otherwise acquiring any interest in shares of our Class A common stock is deemed to have notice of and consented to the foregoing provisions. We recognize that the forum selection clause in our amended and restated certificate of incorporation may impose additional litigation costs on stockholders in pursuing any such claims, particularly if the stockholders do not reside in or near the State of Delaware or the State of Utah, as applicable. Additionally, the forum selection clause in our amended and restated certificate of incorporation may limit our stockholders’ ability to bring a claim in a forum that they find favorable for disputes with us or our directors, officers, or employees, which may discourage such lawsuits against us and our directors, officers, and employees even though an action, if successful, might benefit our stockholders. The Court of Chancery of the State of Delaware or the United States District Court for the District of Utah may also reach different judgments or results than would other courts, including courts where a stockholder considering an action may be located or would otherwise choose to bring the action, and such judgments may be more or less favorable to us than our stockholders. Alternatively, if a court were to find the choice of forum provisions contained in our amended and restated certificate of incorporation to be inapplicable or unenforceable in an action, we may incur additional costs associated with resolving such action in other jurisdictions, which could harm our business, results of operations, and financial condition.
Because the applicability of the exclusive forum provision is limited to the extent permitted by applicable law, we do not intend that the exclusive forum provision would apply to suits brought to enforce any duty or liability created by the Exchange Act or any other claim for which the federal courts have exclusive jurisdiction. We also acknowledge that Section 22 of the Securities Act creates concurrent jurisdiction for federal and state courts over all suits brought to enforce any duty or liability created by the Securities Act or the rules and regulations thereunder and that there is uncertainty as to whether a court would enforce an exclusive forum provision for actions arising under the Securities Act.
Our inability to maintain effective disclosure controls and procedures could adversely affect our results of operations, liquidity and financial positions, as well as our stock price and investor confidence in us.
As a public company, we are subject to certain reporting requirements of the Exchange Act. Our disclosure controls and procedures are designed to reasonably assure that information required to be disclosed by us in reports we file or submit under the Exchange Act is accumulated and communicated to management, recorded, processed, summarized, and reported within the time periods specified in the rules and forms of the SEC. We believe that any disclosure controls and procedures or internal controls and procedures, no matter how well conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met. These inherent limitations include the realities that judgments in decision-making can be faulty, and that breakdowns can occur because of simple error or mistake. Additionally, controls can be circumvented by the individual acts of some persons, by collusion of two or more people or by an unauthorized override of the controls. Accordingly, because of the inherent limitations in our control system, misstatements or insufficient disclosures due to error or fraud may occur and not be detected.
We are not currently eligible to use a short-form Form S-3 registration due to our failure to timely file a current report on Form 8‑K relating to the resignation of one of our named executive officers, which we resolved by the filing of an 8-K on July 31, 2023. As management continues to work with outside counsel to adopt formal training procedures to periodically educate the Company’s officers as to the Company’s SEC reporting responsibilities, our principal executive and principal financial officers have concluded that we had effective disclosure controls and procedures as of December 31, 2023. However, we cannot provide assurance that we will not have further lapses in our disclosure controls and procedures, which could result in our failure to provide accurate and timely disclosure to our investors.
We expect to continue incurring significant costs as a result of operating as a public company, and our management is required to devote substantial time to new compliance initiatives.
As a public company, we expect to continue incurring significant legal, accounting, and other expenses that we did not incur as a private company. We are subject to the reporting requirements of the Exchange Act, which require, among other things that we file with the SEC annual, quarterly, and current reports with respect to our business and financial condition.
In addition, the Sarbanes-Oxley Act, as well as rules subsequently adopted by the SEC and The Nasdaq Global Market to implement provisions of the Sarbanes-Oxley Act, impose significant requirements on public companies, including requiring establishment and maintenance of effective disclosure and financial reporting controls and changes in corporate governance practices. Further, in July 2010, the Dodd-Frank Wall Street Reform and Consumer Protection Act, or the Dodd-Frank Act, was enacted. There are significant corporate governance and executive compensation related provisions in the Dodd-Frank Act concerning areas such as “say on pay” and proxy access. EGCs are permitted to implement many of these requirements over a longer period, which may be up to five years from the pricing of our IPO. Stockholder activism, the current political environment and the current high level of government intervention and regulatory reform may lead to substantial new regulations and disclosure obligations, which may lead to additional compliance costs and impact the manner in which we operate our business in ways we cannot currently anticipate.
Rules and regulations applicable to public companies have substantially increased and are expected to increase our legal and financial compliance costs and to make some activities more time-consuming and costly. If these requirements divert the attention of our management and personnel from other business concerns, they could have an adverse effect on our business. The increased costs will decrease our net income or increase our net loss, and may require us to reduce costs in other areas of our business or increase the prices of our products or services. For example, these rules and regulations make it more difficult and more expensive for us to obtain director and officer liability insurance and we incur substantial costs to maintain the same or similar coverage as when we were a private company. We cannot predict or estimate the amount or timing of additional costs we may incur to respond to these requirements. The impact of these requirements could also make it more difficult for us to attract and retain qualified persons to serve on our board of directors, our board committees or as executive officers.
If we fail to maintain an effective system of internal control over financial reporting, we may not be able to accurately report our financial results or prevent fraud. As a result, stockholders could lose confidence in our financial and other public reporting, which would harm our business and the trading price of our Class A common stock.
Effective internal controls over financial reporting are necessary for us to provide reliable financial reports and, together with adequate disclosure controls and procedures, are designed to prevent fraud. Any failure to implement required new or improved controls, or difficulties encountered in their implementation could cause us to fail to meet our reporting obligations. In addition, any testing by us conducted in connection with Section 404, or any subsequent testing by our independent registered public accounting firm, may reveal deficiencies in our internal controls over financial reporting that are deemed to be material weaknesses or that may require prospective or retroactive changes to our financial statements or identify other areas for further attention or improvement. Inferior internal controls could also cause investors to lose confidence in our reported financial information, which could have a negative effect on the trading price of our stock.
We are required to disclose changes made in our internal controls and procedures on a quarterly basis and our management are required to assess the effectiveness of these controls annually. However, for as long as we are an EGC, our independent registered public accounting firm will not be required to attest to the effectiveness of our internal controls over financial reporting pursuant to Section 404. We could be an EGC for up to five years. An independent assessment of the effectiveness of our internal controls over financial reporting could detect problems that our management’s assessment might not. Undetected material weaknesses in our internal controls over financial reporting could lead to restatements of our financial statements and require us to incur the expense of remediation.
Item 1B. Unresolved Staff Comments
None.
Item 1C. Cybersecurity
Cybersecurity
We recognize the critical importance of maintaining the trust and confidence of stakeholders toward our business and are committed to protecting the confidentiality, integrity, and availability of our business operations and systems. Our board of directors is actively involved in oversight of our risk management activities, and cybersecurity represents an important element of our overall approach to risk management. Our cybersecurity policies, standards, processes, and practices are based on recognized frameworks established by the National Institute of Standards and Technology, or NIST, and other applicable industry standards. In general, we seek to address cybersecurity risks through a comprehensive
approach that is focused on preserving the confidentiality, security, and availability of the information that we collect and store by identifying, preventing, and mitigating cybersecurity threats and effectively responding to cybersecurity incidents when they occur.
Cybersecurity Risk Management and Strategy; Effect of Risk
We face risks related to cybersecurity such as unauthorized access, cybersecurity attacks and other security incidents, loss of data, and misappropriation of confidential information. To identify and assess material risks from cybersecurity threats, we maintain a comprehensive cybersecurity program to ensure our systems are effective and prepared for information security risks, including regular oversight of our programs for security monitoring for internal and external threats to ensure the confidentiality and integrity of our information assets. We consider risks from cybersecurity threats alongside other company risks as part of our overall risk assessment process. We employ a range of tools and services, including third-party real-time risk assessments of cyber assets and mitigation of security risks, data loss prevention, regular air-gapped backups, continuous monitoring and threat response, advanced firewall systems, and security information and event management. As discussed in more detail under “Cybersecurity Governance” below, our audit committee provides oversight of our cybersecurity risk management and strategy processes, which are led by our Chief Information Officer.
We also identify our cybersecurity threat risks by comparing our processes to standards set by NIST. To provide for the availability of critical data and systems, maintain regulatory compliance, manage our material risks from cybersecurity threats, and protect against and respond to cybersecurity incidents, we undertake the following activities:
•monitor emerging data protection best practices and laws and implement changes to our processes that are designed to comply with such;
•annual HIPAA security and privacy risk assessments performed with third party provider, as well as annual HIPAA compliance audits;
•through our policies, practices and contracts (as applicable), require employees, as well as third parties that provide services on our behalf, to treat confidential information and data with care;
•employ technical safeguards that are designed to protect our information systems from cybersecurity threats, including advanced firewall systems, endpoint detection and response, data loss prevention, regular air-gapped backups, and security information and event management, which are evaluated and improved through third-party real-time risk assessments and mitigation of security risks;
•provide regular, mandatory training for our employees and contractors regarding cybersecurity threats as a means to equip them with effective tools, information and education to recognize and address cybersecurity threats;
•conduct regular phishing email simulations for all employees and contractors with access to our email systems to enhance awareness and responsiveness to possible threats;
•leverage the NIST incident handling framework to help us identify, protect, detect, respond and recover when there is an actual or potential cybersecurity incident;
•carry and maintain information security risk insurance that provides protection against the potential losses arising from a cybersecurity incident; and
•document internal policies and procedures for cybersecurity incident response and recovery.
Our incident response plan coordinates the activities we take to prepare for, detect, respond to, and recover from cybersecurity incidents, which include processes to triage, assess severity for, escalate, contain, investigate and remediate the incident, as well as to comply with potentially applicable legal obligations and mitigate damage to our business and reputation.
Our policies and processes also address cybersecurity threat risks associated with our use of third-party service providers. In addition, cybersecurity considerations affect the selection and oversight of our third-party service providers. We perform diligence on third parties that have access to our data to ensure they have adequate cybersecurity safeguards in place and continually monitor cybersecurity threat risks identified through such diligence.
We describe whether and how risks from identified cybersecurity threats, including as a result of any previous cybersecurity incidents, have materially affected or are reasonably likely to materially affect us, including our business strategy, results of operations, or financial condition, under the heading “Security breaches, losses of data, and other disruptions could compromise sensitive information related to our business or prevent us from accessing critical information and expose us to liability, which could adversely affect our business and reputation,” which disclosures are incorporated by reference herein.
Cybersecurity Governance; Management
Cybersecurity is an important part of our risk management processes and an area of focus for our board of directors and management. The audit committee of our board of directors is responsible for the oversight of risks from cybersecurity threats.
At least annually, our audit committee receives an update from management of our cybersecurity threat risk management and strategy processes covering topics such as data security, results from third-party assessments, our incident response plan, and material cybersecurity threat risks or incidents and developments, as well as the steps management has taken to respond to such risks. In such sessions, our audit committee generally receives materials that include a cybersecurity scorecard and other materials discussing current and emerging material cybersecurity threat risks, and describing our ability to mitigate those risks, as well as recent developments, evolving standards, and information security considerations arising with respect to our peers and third parties. The audit committee discusses such matters with our Chief Information Officer.
Our cybersecurity risk management and strategy processes, which are discussed in greater detail above, are led by our Chief Information Officer and the information technology team. Such individuals have extensive experience in various roles, including in other publicly traded companies, involving managing information security, developing cybersecurity strategy, and implementing effective information and cybersecurity programs. These management team members monitor the prevention, mitigation, detection, and remediation of cybersecurity incidents through their management of the cybersecurity risk management and strategy processes described above, including the operation of our incident response plan. As discussed above, these management team members report to the audit committee of our board of directors about cybersecurity threat risks, among other cybersecurity related matters, at least annually.
Item 2. Properties
Our corporate headquarters and facilities are located in Salt Lake City, Utah. We currently lease a total of approximately 24,300 square feet of building space in Salt Lake City dedicated to research and development, administration and our CLIA-certified laboratory. The lease on our existing Salt Lake City facility expires on December 31, 2025 and we have an option to terminate the lease under certain circumstances after July 1, 2024.
Item 3. Legal Proceedings
We are not currently a party to any material litigation or other material legal proceedings. We may, from time to time, be involved in various legal proceedings arising from the normal course of business activities, and an unfavorable resolution of any of these matters could materially affect our future results of operations, cash flows, or financial position.
Item 4. Mine Safety Disclosures
None.
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Information
Our Class A common stock began trading on the Nasdaq Global Market under the symbol “SERA” on July 15, 2021. Prior to that time, there was no public market for our stock. Our Class B common stock is not listed on any stock exchange nor traded on any public market.
Holders of Record
As of March 15, 2024, we had 120 stockholders of record of our Class A common stock. Stockholders of record are defined as those stockholders whose shares are registered in their names in our stock records and do not include beneficial owners of common stock whose shares are held in the names of brokers, dealers or clearing agencies. As of March 15, 2024, we had two stockholders of record of our Class B common stock.
Dividend Policy
We have never declared or paid any cash dividend on our common stock. We intend to retain any future earnings to finance the operation and growth of our business, and we do not anticipate declaring or paying any cash dividends in the foreseeable future.
Unregistered Sales of Securities and Use of Proceeds
None.
Issuer Purchases of Equity Securities
None.
Item 6. [ Reserved ]
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
You should read the following discussion and analysis of our financial condition and results of operations together with our financial statements and related notes appearing elsewhere in this Annual Report on Form 10-K. Some of the information contained in this discussion and analysis or set forth elsewhere in this Form 10-K, including information with respect to our plans and strategy for our business and related financing, includes forward-looking statements that involve risks and uncertainties. As a result of many factors, including those factors set forth in the “Risk Factors” section of this Form 10-K, our actual results could differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
Investors and others should note that we routinely use the Investors section of our website to announce material information to investors and the marketplace. While not all of the information that we post on the Investors section of our website is of a material nature, some information could be deemed to be material. Accordingly, we encourage investors, the media, and others interested in us to review the information that we share on the Investors section of our website, investors.seraprognostics.com.
Overview
We are a women’s health company utilizing our proprietary proteomics and bioinformatics platform, and significant data resources, to improve maternal and neonatal health by discovering, developing, and commercializing blood-based biomarker tests and predictive analytic products and services. Our vision is to deliver pivotal and actionable information to pregnant women, their physicians, and health care payers to significantly enhance a mother’s pregnancy journey, improve maternal and neonatal health, and dramatically reduce health care costs. We believe that our method of combining the disciplines of proteomics and bioinformatics with rigorous clinical testing, data, and economic analysis enables us to
provide physicians, patients, and consumers with personally insightful, clinically meaningful, and economically impactful information designed to improve the pregnancy experience and outcomes for mothers and babies.
There are approximately 140 million births globally each year, and approximately 3.7 million births annually in the United States. Of these, it is estimated that as many as 30% are affected by various complications (i.e., a high-risk pregnancy), including: preterm birth, preeclampsia, fetal growth restriction, stillbirth, hypertension of pregnancy, gestational diabetes, and others. In many cases these complications have profound short- and long-term health consequences for the mother and baby. These health consequences of preterm birth alone are estimated to be approximately $25 billion annually in the United States. This underscores that existing methods to predict adverse pregnancy outcomes are insufficient for timely and effective proactive management for the vast majority of high-risk pregnancies. We believe that positive patient outcomes are the result of appropriate care, and the primary differentiator of patient care should be based on a determination of risk informed by a number of factors including our novel diagnostic tests.
Our first commercial product, the PreTRM test, is the only broadly validated, commercially available blood-based biomarker test to accurately predict the risk of a premature delivery, also known as preterm birth. The PreTRM test is a non-invasive blood test given to a pregnant woman, carrying a single fetus, during weeks 18 through 20 of gestation that provides an accurate prediction of the expectant mother’s risk of delivering spontaneously before 37 weeks’ gestation. Our commercialization strategy includes streamlining patient access to the test by improving specimen acquisition and transport and conducting clinical trials to demonstrate the health and economic benefits of early and accurate detection of preterm birth risk coupled with well-recognized interventions in higher risk patients. Clinical trials conducted to date include the Prediction and Prevention of Preterm Birth, or the PREVENT-PTB Study, Serum Assessment of Preterm Birth Outcomes Compared to Historical Controls study, or the AVERT PRETERM TRIAL, and the Prematurity Risk Assessment Combined With Clinical Interventions for Improving Neonatal outcoMEs study, or the PRIME study. Manuscript results of these studies demonstrate consistency in the reported beneficial impact of the PreTRM test and treat strategy. Specifically, this includes evidence of a prolongation of gestation, shortened hospital or NICU length of stay, and improvements in measures of neonatal morbidity/mortality. A model that is emerging is that by identifying and intervening on at-risk pregnancies, not identifiable by other approaches, babies destined for premature delivery remain in utero longer. This prolongation of gestation in the preterm period leads to more mature babies that require shorter hospital/NICU stays due to improved neonatal health. The PRIME study, for which enrollment was stopped due to efficacy at the interim analysis and is being prepared for publication, includes the same Primary and Secondary outcomes as the AVERT PRETERM TRIAL and affords the continued assessment of this model.
We believe market adoption by both health care providers and payers should be aided by the recent publication of our PREVENT-PTB study sub-analysis, positive data from our AVERT PRETERM TRIAL, our PRIME study, and other real-world evidence studies. We believe the data that will be published over the coming years, together with our current body of evidence, will further demonstrate the clinical and economic utility of our test.
In December 2023, we announced that the Data Safety Monitoring Board, or DSMB, overseeing our PRIME study recommended stopping enrollment due to efficacy, reporting that either co-primary endpoints, neonatal hospital length of stay and composite neonatal morbidity and mortality, met the stopping criteria for statistical significance at the pre-planned interim analysis. We adopted the DSMB’s recommendation and stopped PRIME study enrollment to focus on analyzing and reporting the available data. A manuscript reporting study results, including top-line and exploratory analyses, is being prepared for submission and peer review.
We have built an advanced, proprietary, and scalable proteomics and bioinformatics platform to characterize the biology of pregnancy and to discover and validate key protein biomarkers found in blood that are highly accurate predictors of dynamic changes that occur during pregnancy. By incorporating our proprietary technology platform into our rigorous data-driven development process, we have created a differentiated approach for effectively addressing major milestones, conditions, and features of pregnancy. We believe our large and growing pregnancy dataset (clinical, demographic, proteomic) is a substantial asset for understanding pregnancy complications, health inequities, and the personal pregnancy journey. We envision that our comprehensive approach will enable us to fully characterize one of the most important periods in the lives of women and their babies, and will help to improve their well-being.
We are actively discovering and developing several additional biomarker tests to predict other specific major conditions of pregnancy, such as a pregnancy risk prediction panel test. We believe these tests have the potential to offer significant health benefits to women and their babies. Among other products, we are developing a test designed to provide a more accurate estimate of the delivery date for expectant mothers for the purposes of planning maternity leave, required support, travel arrangements, and related considerations.
Our operations are headquartered in Salt Lake City, Utah, including a CLIA-certified laboratory. Since our inception, we have devoted the majority of our efforts and resources to performing research and development, acquiring product rights, raising capital, establishing facilities, conducting clinical trials, and establishing commercial operations to develop and commercialize the PreTRM test. During this period, we have incurred annual net losses. We have largely funded our operations with proceeds from the sale and issuance of convertible preferred stock, debt financings, bank loans, and the sale and issuance of Class A common stock in our initial public offering, or IPO, which was completed in July 2021.
We have incurred significant operating losses since inception. Our net losses were $36.2 million and $44.2 million for the years ended December 31, 2023 and 2022, respectively. We expect to incur significant additional operating losses and negative cash flows for the foreseeable future, principally as a result of our commercialization activities for the PreTRM test, and to support additional clinical studies, publications, and anticipated research and development of our other pipeline products and services.
We have taken steps to significantly reduce our annual operating expenses across all aspects of our business and we believe our cash runway is sufficient to enable us to operate into 2027 based on our existing operating plans. We will continue to evaluate the allocation of our resources as we focus our efforts to accelerate the market adoption of our PreTRM test and the development and launch of additional pipeline products and services. Our evidence portfolio continues to grow with the publication of a PREVENT-PTB study sub-analysis of the potential benefit of care coordination and low-dose aspirin paired with PreTRM test results. We have finalized the AVERT PRETERM TRIAL primary analysis for peer review, the details of which can be found on the medrxiv pre-print server. Our real-world evidence implementation programs, targeting to expand PreTRM clinical utility data and replicate randomized controlled trial evidence in the real world, have been developed for study launches anticipated in 2024 and 2025.
We will continue to opportunistically negotiate contracts with private and governmental payers and health systems with new positive data from the PREVENT-PTB study, the AVERT PRETERM TRIAL, and the PRIME study, along with real-world evidence studies and other data we plan to generate, and we believe these efforts may eventually result in material revenues. However, if we are unable to secure payer contracts and generate significant market adoption by providers resulting in significant revenues, or if we fail to develop and successfully market our additional tests that generate additional revenues, we may be required to delay, scale back or abandon some, or all, of our development programs and other operations. Until such time as we can generate significant revenue from the sales of our products, if ever, we may need to continue to finance our cash needs through equity offerings, debt financings or other capital sources, potentially including collaborations or other similar arrangements. Debt financing and preferred equity financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making acquisitions or capital expenditures or declaring dividends and may require the issuance of warrants. If we raise additional funds through collaborations, strategic alliances or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, or product candidates or grant licenses on terms that may not be favorable to us. If we are unable to raise additional funds through equity or debt financings when needed, we may have to significantly delay, reduce, or eliminate some or all of our product development or future commercialization efforts, or grant rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves. Our ability to access capital when needed is not assured and, if not achieved on a timely basis, will materially harm our business, financial condition, and results of operations.
Factors Affecting Our Performance
We believe there are several important factors that have impacted, and that we expect will continue to impact, our operating performance and results of operations, including:
•our ability to further increase the use and adoption of the PreTRM test;
•our ability to develop and successfully commercialize new products and services in the future;
•the continued development of the market for proteomics and bioinformatics;
•our ability to secure payer and health system contracts that result in significant revenues or to access additional funds;
•raising substantial additional capital to continue operations and execute on our business plan, until such time as we can generate significant revenue from the sales of our products, if ever;
•obtaining and maintaining intellectual property protection for our technology and products; and
•other factors described in the “Risk Factors” section and elsewhere in this report.
Key Components of Our Results of Operations
Revenues
Substantially all of our revenue in the near term is expected to come from sales of the PreTRM test. We expect to derive future revenues from PreTRM and other pipeline tests. As we continue to engage with payers and health systems using our latest evidence, we aim to close additional contracts which would eventually result in additional revenues when health care providers order the PreTRM test. We believe market adoption by both health care providers and payers could be aided by the PREVENT-PTB study sub-analysis, the publication of the AVERT PRETERM TRIAL results, the publication of positive PRIME study interim data, and other evidence generated within the next three years. We believe market accessibility of the test could be improved by our progress toward diversifying our specimen collection methods and enhanced awareness and engagement with patients. Revenue from our other pipeline products and services is expected to be dependent on our ability to successfully market them to patients, providers, payers, and, in most cases, a combination of the three.
Operating Expenses
Cost of Revenue
Cost of revenue reflects the aggregate costs incurred in delivering the proteomic testing results to clinicians and includes expenses for third-party specimen collection and shipping costs, as well as our lab personnel, materials and supplies, equipment, and infrastructure expenses associated with clinical testing, and allocated overhead including rent and equipment depreciation. Some of these components can vary significantly in cost and reliability of supply, and we periodically seek ways to make our supplier network more robust. For example, to address the risk posed by potential disruptions in specimen collection services described in the “Risk Factors” section of this report, we are working to engage alternative specimen collection providers beyond those that have traditionally supplied the majority of our needs. We expect costs of revenue will generally move in line with the sales of the PreTRM test.
Research and Development Expenses
Research and development expenses consist of costs incurred for our research activities and development of our product candidates. These expenses include:
•clinical and real-world studies;
•laboratory processes;
•research and bioinformatic activities;
•biobanking and publication efforts;
•personnel-related expenses, including salaries, payroll taxes, employee benefits, and stock-based compensation charges for employees engaged in these research and development activities;
•direct study expenses incurred under agreements with study sites or contract research organizations;
•consultants engaged in our research and development efforts;
•laboratory materials and supplies;
•facilities costs; and
•depreciation, amortization, and other direct and allocated expenses, including insurance and other operating costs, incurred as a result of our research and development activities.
We expense all research and development costs, both internal and external, in the period in which they are incurred. We expect that our research and development expenses will decrease slightly in 2024 compared to 2023 due to the PRIME study stopping enrollment due to efficacy at the end of 2023. Research and development costs may increase in the medium to long-term as we support current and additional clinical studies, publications, and other product development activities.
Selling and Marketing Expenses
Selling and marketing expenses consist primarily of salaries, payroll taxes, employee benefits, and stock-based compensation charges for sales, marketing, and payer access personnel. Other significant costs include travel, consulting, public relations, facilities, and legal costs related to commercial efforts. We expect selling and marketing expenses will decrease in 2024 compared to 2023 as we recently took steps to further streamline our near-term commercial strategy to refocus on institutional sales as we generate additional clinical data. We expect selling and marketing expenses to increase in the medium to long-term as we expand our commercial efforts as opportunity dictates and increase our product portfolio.
General and Administrative Expenses
General and administrative expenses consist primarily of salaries, payroll taxes, employee benefits, and stock-based compensation charges for personnel in executive, finance, information technology, human resources, and other administrative functions. Other significant costs include facilities, corporate and intellectual property legal fees, accounting, insurance, consulting, and other professional fees.
We expect general and administrative expenses in 2024 could remain consistent or decrease slightly compared to 2023, but such expenses could increase in the medium to long-term as needed to support future operations and anticipated revenue growth.
Interest Expense
Interest expense represents interest incurred on our finance leases.
Other Income, Net
Other income, net consists of interest income and other investment income earned on our cash, cash equivalents, and marketable securities, and other gains and losses.
Results of Operations
The results of operations presented below should be reviewed in conjunction with the financial statements and related notes included elsewhere in this report.
Comparison of the Years Ended December 31, 2023 and 2022
The following table summarizes our results of operations for the years ended December 31, 2023 and 2022:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2023 | | 2022 | | $ Change |
| (in thousands) |
| Revenue | $ | 306 | | | $ | 268 | | | $ | 38 | |
| Operating expenses: | | | | | |
| Cost of revenue | 210 | | | 193 | | | 17 | |
| Research and development | 15,225 | | | 14,244 | | | 981 | |
| Selling and marketing | 8,349 | | | 14,699 | | | (6,350) | |
| General and administrative | 16,343 | | | 16,784 | | | (441) | |
| Total operating expenses | 40,127 | | | 45,920 | | | (5,793) | |
| Loss from operations | (39,821) | | | (45,652) | | | 5,831 | |
| Interest expense | (55) | | | (61) | | | 6 | |
| Other income, net | 3,634 | | | 1,527 | | | 2,107 | |
| Net loss | $ | (36,242) | | | $ | (44,186) | | | $ | 7,944 | |
Research and Development Expenses
The following table summarizes our research and development expenses for the years ended December 31, 2023 and 2022:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2023 | | 2022 | | $ Change |
| (in thousands) |
| Research and development expenses: | | | | | |
| Clinical studies | $ | 6,784 | | | $ | 5,818 | | | $ | 966 | |
| Research and bioinformatics | 4,412 | | | 4,312 | | | 100 | |
| Laboratory operations | 4,029 | | | 4,114 | | | (85) | |
| Total research and development expenses | $ | 15,225 | | | $ | 14,244 | | | $ | 981 | |
The $1.0 million increase was due to a $1.0 million increase in clinical study costs, and a $0.1 million increase in research and bioinformatics expenses, partially offset by a $0.1 million decrease in laboratory operations costs. The $1.0 million increase in clinical study costs was primarily due to a $1.3 million increase resulting from the increased activity in the PRIME study and a $0.1 million increase in consulting costs, partially offset by a $0.5 million decrease in personnel costs driven by decreased average headcount. The $0.1 million increase in research and bioinformatics expenses was primarily due to an increase of $0.3 million in personnel costs driven by increased average headcount, partially offset by a $0.2 million decrease in specimen acquisition costs related to product development. The $0.1 million decrease in laboratory operations costs was primarily due to a $0.4 million decrease in personnel costs driven by decreased average headcount and a $0.3 million decrease in lab supplies, partially offset by a $0.5 million increase related to lab equipment and associated depreciation.
Selling and Marketing Expenses
The $6.4 million decrease was due primarily to decreases of $4.3 million in personnel-related costs driven by decreased average headcount, $0.8 million of travel costs driven by decreased average headcount, $0.7 million of marketing programs and materials development, $0.5 million of consulting and outside services, and $0.4 million of IT systems supporting sales efforts. These decreases are largely a result of steps we took to further streamline our near-term commercial strategy to refocus on institutional sales as we generate additional clinical data.
General and Administrative Expenses
The $0.4 million decrease was due primarily to decreases of $0.8 million of director and officer insurance costs and $0.8 million of personnel expenses driven by decreased average headcount, partially offset by increases of $0.8 million related to one-time personnel costs and $0.3 million of legal expenses.
Other Income, net
The $2.1 million increase in other income was due to a $1.2 million increase related primarily to investment income on our marketable securities and a $0.9 million increase in interest income related primarily to our marketable securities.
Liquidity and Capital Resources
Sources of Liquidity
Since inception, we have not generated a significant amount of commercial revenue from product sales or any other sources and have incurred significant operating losses and negative cash flows from operations. We anticipate that we will continue to incur net losses for the foreseeable future. We have financed our operations primarily through proceeds from the sale and issuance of convertible preferred stock and convertible notes, bank loans, and the sale and issuance of Class A common stock in our IPO, which was completed in July 2021. As of December 31, 2023, we had aggregate cash, cash equivalents, and available-for-sale securities of $79.9 million, and an accumulated deficit of $246.9 million.
Cash Flows
The following table summarizes our cash flows for the periods indicated:
| | | | | | | | | | | |
| Year Ended December 31, |
| 2023 | | 2022 |
| (in thousands) |
| Net cash (used in) provided by: | | | |
| Operating activities | $ | (27,188) | | | $ | (34,610) | |
| Investing activities | 438 | | | 5,551 | |
| Financing activities | 752 | | | 5 | |
| Net decrease in cash and cash equivalents | $ | (25,998) | | | $ | (29,054) | |
Operating Activities
The net cash used in operating activities during the year ended December 31, 2023 was primarily due to a net loss of $36.2 million, partially offset by non-cash charges of $5.5 million and an increase in operating assets and liabilities of $3.5 million. The net cash used in operating activities during the year ended December 31, 2022 was primarily due to a net loss of $44.2 million, partially offset by non-cash charges of $6.0 million and an increase in operating assets and liabilities of $3.6 million.
Investing Activities
Net cash provided by investing activities for the year ended December 31, 2023 was primarily due to $54.4 million in proceeds from maturities and sales of marketable securities, partially offset by $54.1 million in purchases of marketable securities. Net cash used in investing activities for the year ended December 31, 2022 was primarily due to $54.4 million in proceeds from maturities and sales of marketable securities, partially offset by $48.1 million in purchases of marketable securities and $0.8 million in purchases of property and equipment.
Financing Activities
Net cash provided by financing activities for the year ended December 31, 2023 was due to $1.2 million in proceeds from employee equity transactions, partially offset by $0.5 million of finance lease principal payments. Net cash provided by financing activities for the year ended December 31, 2022 was due to $0.3 million in proceeds from options exercised, partially offset by $0.3 million of finance lease principal payments.
Future Funding Requirements
We expect to incur significant additional operating losses and negative cash flows for the foreseeable future. We expect our losses in the future to arise principally as a result of our commercialization activities for the PreTRM test and the development, commercialization, marketing, and distribution of our other pipeline products and services, especially the costs of our PRIME study and additional evidence-generating initiatives. There can be no assurance that we will eventually achieve significant revenues or profitability, or if achieved, can sustain either on a continuing basis. If we are unable to achieve significant revenues or raise additional funding, when needed, we may not be able to continue the development or commercialization of our products and services and could be required to delay, scale back, or abandon some or all of our development programs and other operations. No assurance can be given that we will be successful in raising the required capital at reasonable cost and at the required times, or at all. Any additional equity financing may not be available on favorable terms, most likely will be dilutive to our current stockholders, and debt financing, if available, may involve restrictive covenants and dilutive financing instruments. Further, our operating plan may change, and we may need additional funds to meet operational needs and capital requirements for product development and commercialization sooner than planned. We currently have no credit facility or committed sources of capital. Our future funding requirements will depend on many factors, including the following:
•the timing, receipt, and amount of sales from the PreTRM test and other pipeline products and services, if approved;
•the cost and timing of establishing sales, marketing, and other commercialization capabilities in the United States and abroad;
•our ability to develop and commercialize other products and services;
•the terms and timing of any collaborative, licensing, and other arrangements that we may establish;
•the cost, timing, and outcomes of regulatory approvals;
•the scope, rate of progress, results, and cost of our clinical, scientific, and real-world studies, and other related activities;
•the cost of preparing, filing, prosecuting, defending, and enforcing any patent claims and other intellectual property rights;
•the extent to which we acquire or invest in businesses, products or technologies, although we currently have no commitments or agreements relating to any of these types of transactions;
•partnerships and other strategic options for our PreTRM test and other product candidates; and
•other factors described in the “Risk Factors” section and elsewhere in this report.
We evaluated that our existing cash and cash equivalents will enable us to fund our operating expenses and capital expenditure requirements for at least the next 12 months.
Contractual Obligations and Commitments
Our material cash requirements include the following contractual and other obligations.
Leases
We have lease arrangements for certain equipment and facilities. As of December 31, 2023, we had future minimum lease payments of $2.0 million, with $1.1 million payable within 12 months.
Consulting Agreement
We have a consulting agreement with Blue Ox Healthcare Partners, LLC, or Blue Ox, to advise us on development of strategies with the goal to obtain widespread insurance coverage for the PreTRM test. As of December 31, 2023, we had future minimum payments under this agreement of $0.7 million, which is payable within 12 months.
Critical Accounting Policies and Estimates
Our management’s discussion and analysis of financial condition and results of operations is based on our financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles. The preparation of these financial statements requires us to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements, as well as the reported revenue and expenses incurred during the reporting periods. Our estimates are based on our historical experience and on various other factors that we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions. We believe that the accounting policies discussed below are critical to understanding our historical and future performance, as these policies relate to the more significant areas involving management’s judgments and estimates.
Stock-based Compensation
We maintain a stock-based compensation plan as a long-term incentive for employees and non-employee consultants. The plan allows for the issuance of incentive stock options and non-qualified stock options, as well as other stock rights.
We recognize stock-based compensation expense for stock options on a straight-line basis over the requisite service period and estimate forfeitures based on historical evidence. Our stock-based compensation expenses are based upon the grant date fair value of options estimated using the Black-Scholes option pricing model. Input assumptions used in calculating the fair value of stock-based awards represent management’s estimates and involve inherent uncertainties and
the application of management’s judgment. These input assumptions include the expected term of the awards, the expected common stock price volatility over the term of the awards, risk-free interest rates, and the expected dividend yield. Changes in the assumptions can materially affect the fair value and ultimately how much stock-based compensation expense is recognized. We will continue to use judgment in evaluating the expected volatility, expected terms, and interest rates utilized for our stock-based compensation expense calculations on a prospective basis.
Emerging Growth Company and Smaller Reporting Company Status
We are an emerging growth company, or EGC, as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act. We elected to use the extended transition period for complying with new or revised accounting standards that have different effective dates for public and private companies until the earlier of the date that we (1) are no longer an EGC or (2) affirmatively and irrevocably opt out of the extended transition period provided in the JOBS Act. Under the JOBS Act, emerging growth companies can delay adopting new or revised accounting standards issued subsequent to the enactment of the JOBS Act until such time as those standards apply to private companies, reduce disclosure obligations regarding executive compensation in our periodic reports and proxy statements, and are exempt from the requirements of holding a nonbinding advisory vote on executive compensation and any golden parachute payments not previously approved. As an EGC, we are also not required to have our internal control over financial reporting audited by our independent registered public accounting firm pursuant to Section 404 of the Sarbanes-Oxley Act. As a result, our financial statements may not be comparable to companies that comply with the new or revised accounting pronouncements as of public company effective dates and we are not required to provide auditor attestation regarding requirements of Section 404(b) of Sarbanes-Oxley.
We will remain an EGC until the earliest to occur of: (1) the last day of the fiscal year in which we have at least $1.235 billion in annual revenue; (2) the last day of the fiscal year in which we are deemed to be a “large accelerated filer,” as defined in Rule 12b-2 under the Exchange Act, which would occur if the market value of our common stock held by non-affiliates exceeded $700.0 million as of the last business day of the second fiscal quarter of such year; (3) the date on which we have issued more than $1.0 billion in non-convertible debt securities during the prior three-year period; and (4) December 31, 2026.
We are also a “smaller reporting company” as defined in the Exchange Act. We may continue to be a smaller reporting company even after we are no longer an emerging growth company. We may take advantage of certain of the scaled disclosures available to smaller reporting companies until the fiscal year following the determination that the market value of our voting and non-voting common stock held by non-affiliates is more than $250 million measured on the last business day of our second fiscal quarter, or our annual revenues are less than $100 million during the most recently completed fiscal year and the market value of our voting and non-voting common stock held by non-affiliates is more than $700 million measured on the last business day of our second fiscal quarter.
Recent Accounting Pronouncements
A description of recent accounting pronouncements that may potentially impact our financial position, results of operations or cash flows is disclosed in Note 2—Significant Accounting Policies, appearing in Part II, Item 8 of this Annual Report on Form 10-K.
Item 7A. Quantitative and Qualitative Disclosures about Market Risk
Interest Rate Risk
Our exposure to changes in interest rates relates primarily to interest earned and market value on our cash and cash equivalents and marketable securities.
Our cash and cash equivalents and marketable securities consist of cash held in banks, money market funds, commercial paper, U.S. government securities, U.S. federal agency securities and investment grade corporate securities. Our investment policy and strategy are focused on preservation of capital and supporting our liquidity requirements. Changes in U.S. interest rates affect the interest earned on our cash and cash equivalents and marketable securities, and the market value of those securities. A hypothetical 100 basis point increase in interest rates would have resulted in a decrease of $0.6 million in the market value of our available-for-sale debt securities as of December 31, 2023. Any realized gains or losses resulting from such interest rate changes would only occur if we sold the investments prior to maturity. We do not
intend to sell investments while they are in an unrealized loss position and do not believe we will be required to sell the investments before recovery, which may be maturity.
Foreign Currency
We do not regularly incur expenses with vendors outside the United States or that are denominated in currencies other than the U.S. dollar. We may incur such expenses in the future at which point exchange rate fluctuations might adversely affect our expenses, results of operations, financial position and cash flows. To date, exchange rate fluctuations have not had a material effect on our results of operations.
Effects of Inflation
We do not believe inflation has had a material effect on our results of operations during the periods presented. However, the current inflationary environment could affect us by increasing our costs of labor, laboratory supplies, and clinical trials and could adversely affect our business, results of operations, financial position and cash flows. In addition, increased inflation has had, and may continue to have, an effect on interest rates and may adversely affect our borrowing rate and our ability to obtain any potential additional funding.
Item 8. Financial Statements and Supplementary Data
INDEX TO FINANCIAL STATEMENTS
Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of Sera Prognostics, Inc.
Opinion on the Financial Statements
We have audited the accompanying balance sheets of Sera Prognostics, Inc. (the Company) as of December 31, 2023 and 2022, the related statements of operations and comprehensive loss, stockholders’ equity and cash flows for each of the two years in the period ended December 31, 2023, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2023 and 2022, and the results of its operations and its cash flows for each of the two years in the period ended December 31, 2023, in conformity with U.S. generally accepted accounting principles.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Ernst & Young LLP
We have served as the Company’s auditor since 2012.
Salt Lake City, Utah
March 20, 2024
SERA PROGNOSTICS, INC.
Balance Sheets
(in thousands, except share and per share data)
| | | | | | | | | | | |
| December 31, |
| 2023 | | 2022 |
| Assets | | | |
| Current assets: | | | |
| Cash and cash equivalents | $ | 3,880 | | | $ | 29,878 | |
| Marketable securities | 45,199 | | | 52,826 | |
| Accounts receivable | 160 | | | 113 | |
| Other receivables | 11,310 | | | 6,000 | |
| Prepaid expenses and other current assets | 795 | | | 1,308 | |
| Total current assets | 61,344 | | | 90,125 | |
| Property and equipment, net | 1,999 | | | 3,059 | |
| Long-term marketable securities | 30,841 | | | 21,329 | |
| Other assets | 1,257 | | | 1,816 | |
| Total assets | $ | 95,441 | | | $ | 116,329 | |
| Liabilities and Stockholders' Equity | | | |
| Current liabilities: | | | |
| Accounts payable | $ | 1,046 | | | $ | 1,548 | |
| Accrued and other current liabilities | 2,722 | | | 4,444 | |
| Finance lease obligation, current portion | 440 | | | 464 | |
| Deferred revenue | 20,235 | | | 9,082 | |
| Total current liabilities | 24,443 | | | 15,538 | |
| Finance lease obligation, net of current portion | 196 | | | 626 | |
| Operating lease obligation, net of current portion | 644 | | | 1,222 | |
| Total liabilities | 25,283 | | | 17,386 | |
| Commitments and contingencies (Note 12) | | | |
| Stockholders' equity: | | | |
| Common stock, $0.0001 par value; 150,000,000 Class A shares authorized; 30,736,513 and 29,612,687 Class A shares issued and outstanding as of December 31, 2023 and 2022, respectively; 1,500,000 Class B shares authorized; 1,405,259 Class B shares issued as of December 31, 2023 and 2022; 967,759 and 1,405,259 Class B shares outstanding as of December 31, 2023 and 2022, respectively. | 3 | | | 3 | |
| Additional paid-in capital | 317,066 | | | 310,575 | |
| Accumulated other comprehensive loss | (15) | | | (981) | |
| Accumulated deficit | (246,896) | | | (210,654) | |
| Total stockholders' equity | 70,158 | | | 98,943 | |
| Total liabilities and stockholders' equity | $ | 95,441 | | | $ | 116,329 | |
The accompanying notes are an integral part of the financial statements
SERA PROGNOSTICS, INC.
Statements of Operations and Comprehensive Loss
(in thousands, except share and per share data)
| | | | | | | | | | | |
| Year Ended December 31, |
| 2023 | | 2022 |
| Revenue | $ | 306 | | | $ | 268 | |
| Operating expenses: | | | |
| Cost of revenue | 210 | | | 193 | |
| Research and development | 15,225 | | | 14,244 | |
| Selling and marketing | 8,349 | | | 14,699 | |
| General and administrative | 16,343 | | | 16,784 | |
| Total operating expenses | 40,127 | | | 45,920 | |
| Loss from operations | (39,821) | | | (45,652) | |
| Interest expense | (55) | | | (61) | |
| Other income, net | 3,634 | | | 1,527 | |
| Net loss | $ | (36,242) | | | $ | (44,186) | |
| Net loss per share, basic and diluted | $ | (1.16) | | | $ | (1.43) | |
| Weighted-average shares of common stock outstanding, basic and diluted | 31,200,652 | | | 30,943,426 | |
| Other comprehensive income (loss): | | | |
| Unrealized gain (loss) on available-for-sale debt securities | $ | 966 | | | $ | (798) | |
| Total other comprehensive income (loss) | 966 | | | (798) | |
| Comprehensive loss | $ | (35,276) | | | $ | (44,984) | |
The accompanying notes are an integral part of the financial statements
SERA PROGNOSTICS, INC.
Statements of Stockholders’ Equity
(in thousands, except share data)
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Common Stock
(Class A and B) | | Additional
Paid-In
Capital | | Accumulated Other Comprehensive Loss | | Accumulated
Deficit | | Total
Stockholders'
Equity |
| Shares | | Amount | | | | |
| Balance as of December 31, 2021 | 30,774,126 | | | $ | 3 | | | $ | 305,212 | | | $ | (183) | | | $ | (166,468) | | | $ | 138,564 | |
| Issuance of common stock upon exercise of stock options | 243,820 | | | — | | | 308 | | | — | | | — | | | 308 | |
| Stock-based compensation expense | — | | | — | | | 5,055 | | | — | | | — | | | 5,055 | |
| Other comprehensive loss | — | | | — | | | — | | | (798) | | | — | | | (798) | |
| Net loss | — | | | — | | | — | | | — | | | (44,186) | | | (44,186) | |
| Balance as of December 31, 2022 | 31,017,946 | | | $ | 3 | | | $ | 310,575 | | | $ | (981) | | | $ | (210,654) | | | $ | 98,943 | |
| Issuance of common stock upon exercise of stock options | 593,091 | | | — | | | 1,095 | | | — | | | — | | | 1,095 | |
| Issuance of common stock under employee stock purchase plan | 93,235 | | | — | | | 123 | | | — | | | — | | | 123 | |
| Stock-based compensation expense | — | | | — | | | 5,273 | | | — | | | — | | | 5,273 | |
| Other comprehensive income | — | | | — | | | — | | | 966 | | | — | | | 966 | |
| Net loss | — | | | — | | | — | | | — | | | (36,242) | | | (36,242) | |
| Balance as of December 31, 2023 | 31,704,272 | | | $ | 3 | | | $ | 317,066 | | | $ | (15) | | | $ | (246,896) | | | $ | 70,158 | |
The accompanying notes are an integral part of the financial statements
SERA PROGNOSTICS, INC.
Statements of Cash Flows
(in thousands)
| | | | | | | | | | | |
| Year Ended
December 31, |
| 2023 | | 2022 |
| Cash flows from operating activities | | | |
| Net loss | $ | (36,242) | | | $ | (44,186) | |
| Adjustments to reconcile net loss to net cash used in operating activities: | | | |
| Depreciation and amortization | 900 | | | 756 | |
| Stock-based compensation | 5,273 | | | 5,055 | |
| Non-cash lease expense | 526 | | | 462 | |
| Non-cash interest expense | — | | | 12 | |
| Non-cash investment income, net | (1,182) | | | (239) | |
| Other | 18 | | | (22) | |
| Changes in operating assets and liabilities: | | | |
| Accounts receivable | (47) | | | (86) | |
| Other receivables | (5,310) | | | (2,884) | |
| Prepaid expenses and other assets | 465 | | | 718 | |
| Accounts payable | (442) | | | 352 | |
| Accrued and other current liabilities | (2,301) | | | (514) | |
| Deferred revenue | 11,154 | | | 5,966 | |
| Net cash used in operating activities | (27,188) | | | (34,610) | |
| Cash flows from investing activities | | | |
| Purchases of marketable securities | (54,143) | | | (48,073) | |
| Proceeds from maturities and sales of marketable securities | 54,398 | | | 54,399 | |
| Purchases of property and equipment | (128) | | | (791) | |
| Proceeds from disposal of property and equipment | 311 | | | 16 | |
| Net cash provided by investing activities | 438 | | | 5,551 | |
| Cash flows from financing activities | | | |
| Proceeds from exercise of stock options | 1,095 | | | 308 | |
| Proceeds from employee stock purchase plan | 123 | | | — | |
| Finance lease principal payments | (466) | | | (303) | |
| Net cash provided by financing activities | 752 | | | 5 | |
| Net decrease in cash and cash equivalents | (25,998) | | | (29,054) | |
| Cash and cash equivalents at beginning of period | 29,878 | | | 58,932 | |
| Cash and cash equivalents at end of period | $ | 3,880 | | | $ | 29,878 | |
| Supplemental disclosure of cash flow information | | | |
| Cash paid for interest | $ | 55 | | | $ | 48 | |
| Supplemental disclosure of non-cash investing and financing information | | | |
| Purchases of property and equipment in accounts payable and accruals | $ | 20 | | | $ | — | |
The accompanying notes are an integral part of the financial statements
SERA PROGNOSTICS, INC.
Notes to Financial Statements
1. Description of Business and Financial Condition
Sera Prognostics, Inc. (the “Company”) is a women’s health company utilizing its proprietary proteomics and bioinformatics platform to discover, develop, and commercialize biomarker tests with an initial focus on improving pregnancy outcomes. The Company was incorporated in the State of Delaware on January 17, 2008 and its operations are located in Salt Lake City, Utah, including a Clinical Laboratory Improvement Amendments (“CLIA”)-certified laboratory.
Since its inception, the Company’s activities have consisted of performing research and development, conducting clinical studies for its pipeline products and services, acquiring product rights, raising capital, establishing facilities, and organizing commercial operations to market the PreTRM test.
Liquidity and Capital Resources
The accompanying financial statements have been prepared on a going concern basis, which contemplates the realization of assets and the satisfaction of liabilities and commitments in the normal course of business.
The Company has incurred net losses and negative cash flows from operations since inception and had an accumulated deficit of $246.9 million as of December 31, 2023. The Company’s management expects the Company to incur significant additional operating losses and negative cash flows for the foreseeable future, principally as a result of the Company’s activities relating to the PreTRM test and the Company’s other pipeline products and services, including clinical and preclinical trials and anticipated research and development activities as well as commercialization activities. There can be no assurance that the Company will eventually achieve significant revenues or profitability to sustain operations, or if achieved, can sustain either on a continuing basis. If the Company is unable to achieve significant revenues or raise additional funds, when needed, it may not be able to continue the development or commercialization of its products and services and could be required to delay, scale back, or abandon some or all of its operations. No assurance can be given that the Company will be successful in raising the required capital on reasonable terms and at the required times, or at all. Any additional equity financing, if available to the Company, may not be available on favorable terms and may be dilutive to current stockholders, and any debt financing, if available, may involve restrictive covenants and dilutive financing instruments. The Company’s future operations are highly dependent on a combination of factors, including (i) the commercialization and market acceptance of the PreTRM test and the successful development, commercial launch, marketing, and distribution of other pipeline products and services; (ii) the success of scientific and clinical studies and other research and development programs that support current and future products and services; (iii) the development of competitive products by other biotechnology and laboratory companies; (iv) the Company’s ability to manage growth of the organization; (v) the Company’s ability to protect its intellectual property, technology, and products; and, ultimately (vi) the timely and successful completion of any additional financing.
The principal sources of the Company’s working capital to date have been the proceeds from the sale and issuance of convertible preferred stock and convertible notes, bank loans, and the sale and issuance of Class A common stock in an initial public offering (“IPO”), which was completed in July 2021. As of December 31, 2023, the Company had aggregate cash, cash equivalents, and available-for-sale securities of approximately $79.9 million. See Note 3—Cash, Cash Equivalents and Marketable Securities.
The Company evaluated that its existing financial resources are sufficient to continue operating activities at least 12 months from the issuance date of these financial statements.
2. Significant Accounting Policies
Basis of Presentation
The accompanying financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America (“U.S. GAAP”). Any reference in these notes to applicable accounting guidance is meant to refer to the authoritative U.S. GAAP included in the Accounting Standards Codification (“ASC”), and Accounting Standards Updates (“ASU”) issued by the Financial Accounting Standards Board (“FASB”).
Use of Estimates
The preparation of the financial statements in conformity with U.S. GAAP requires the Company’s management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. The Company evaluates these estimates on an ongoing basis. The Company bases these estimates on historical and anticipated results, trends, and various other assumptions that the Company believes are reasonable under the circumstances, including assumptions as to future events. Actual results could differ materially from those estimates.
The Company’s financial statements as of and for the year ended December 31, 2023 reflect the Company’s estimates of the impact of the current macroeconomic environment, including the impact of inflation and higher interest rates. The extent to which these conditions will directly or indirectly impact the Company’s business, results of operations, and financial condition is uncertain. The Company is not aware of any specific event or circumstance that would require an update to its estimates, judgments, and assumptions or a revision of the carrying value of the Company’s assets or liabilities as of the date of this filing.
Cash and cash equivalents
The Company considers all highly liquid financial instruments with maturities of 90 days or less at the date of purchase to be cash equivalents. The carrying amounts reported in the balance sheets for cash and cash equivalents are valued at cost, which approximates their fair value. As of December 31, 2023 and 2022, cash and cash equivalents consisted of cash, money market funds, and commercial paper. Cash and cash equivalents are stated at fair value.
Marketable Securities
The Company has classified its marketable securities, all of which are debt securities, as available-for-sale securities. These securities are carried at estimated fair value. Available-for-sale debt securities with an estimated fair value below the amortized cost basis are assessed to determine what amount of that difference, if any, is attributable to expected credit losses. An allowance for credit losses on available-for-sale debt securities is recognized as a charge in other income, net on the Company’s statements of operations and comprehensive loss, and any remaining unrealized losses, net of the related tax effect, are included in accumulated other comprehensive loss in stockholders’ equity until realized. Gains and losses on marketable security transactions are reported on the specific-identification method.
Concentration of credit risk
Financial instruments that potentially subject the Company to concentrations of credit risk consist primarily of cash and cash equivalents and marketable securities. The Company maintains bank deposits in accounts at federally insured financial institutions and these deposits may exceed federally insured limits. The Company is exposed to credit risk in the event of default by the financial institution holding its cash to the extent recorded in the balance sheet. The Company has not experienced any losses on its deposits of cash. The Company’s cash equivalents consist of money market funds and investment grade commercial paper. Marketable securities consist of investments in U.S. government securities, U.S. federal agency securities, investment grade commercial paper, and investment grade corporate securities. The Company’s investment portfolio in corporate debt securities is highly liquid and diversified among individual issuers. The Company did not experience any credit losses related to its investment portfolio for the years ended December 31, 2023 and 2022.
Property and Equipment
Property and equipment are recorded at cost less accumulated depreciation and amortization. Depreciation and amortization are computed using the straight-line method over the shorter of estimated useful lives of the assets or the respective lease term. The estimated useful life of each asset category is as follows:
| | | | | |
| Computer equipment | 3 years |
| Software | 3 years |
| Machinery and equipment | 5 years |
| Furniture and fixtures | 5 years |
| Leasehold improvements | Shorter of useful life or remaining lease term |
Amortization expense of assets acquired through finance leases is included in depreciation and amortization expense in the accompanying statements of operations and comprehensive loss. Costs of repairs and maintenance that do not extend the useful life or improve the related assets are expensed as incurred. Costs of major replacements or improvements are capitalized. When assets are sold, or otherwise disposed of, the cost and related accumulated depreciation are removed from the accounts and any gain or loss is included in operating expense.
Leases
The Company’s operating lease relates to office and laboratory space at its headquarters. The Company’s finance leases are for certain equipment related to the Company’s information technology infrastructure and laboratory operations. The Company determines if an arrangement is a lease at inception. The Company has elected not to separate lease components from non-lease components for all classes of leased assets except for building leases.
The Company elected to treat leases with lease terms of 12 months or less as short-term leases. No right-of-use assets or lease liabilities are recognized for short-term leases. For leases with a lease term greater than 12 months, right-of-use assets and lease liabilities are recognized on the balance sheets at the commencement date based on the present value of the remaining lease payments and includes only payments that are fixed and determinable at commencement. The Company’s lease terms may include options to extend or terminate when it is reasonably certain that the Company will exercise such options.
To date, the rates implicit in the Company’s finance leases have been determinable, and the Company uses those rates to calculate the present value of its finance lease liabilities. The implicit rate in the Company’s operating lease is not readily determinable. As such, the Company uses its incremental borrowing rate to calculate the present value of its operating lease liabilities.
Operating lease costs are recognized on a straight-line basis over the lease terms. Finance lease assets are amortized on a straight-line basis over the shorter of the estimated useful lives of the assets or the lease terms.
Deferred Revenue
The Company recognizes deferred revenue in accordance with ASC 606, Revenue from Contracts with Customers (“ASC 606”). Deferred revenue is recognized when a customer pays consideration, or the Company has a right to an amount of consideration that is unconditional before the Company transfers the good or service to the customer. The Company’s deferred revenue balance as of December 31, 2023 and 2022 relates to certain contractual minimum payments received by the Company as part of its commercial collaboration agreements. Deferred revenue is recognized as revenue when the Company delivers PreTRM test results to customers pursuant to its commercial collaboration agreements.
Revenue Recognition
Revenue is generated from the sale of PreTRM tests. The Company recognizes revenue based on accounting standards applied to determine the measurement of revenue and timing of when it is recognized. The Company applies the following five-step approach as set forth under ASC 606: (i) identify the contract(s) with a customer; (ii) identify the performance obligations in the contract (iii) determine the transaction price; (iv) allocate the transaction price to the performance obligations in the contract; and (v) recognize revenue when (or as) the Company satisfies a performance obligation. The Company applies the five-step model when it is probable that the Company will collect the consideration it is entitled to in exchange for fulfilling its performance obligation. The Company recognizes revenue upon delivery of test results, which it considers to be the only performance obligation, and allocates all of the transaction price to this performance obligation.
In determining the transaction price, which is an estimate of the amount of variable consideration expected to be received, the Company uses the expected value method under ASC 606. The Company considers all reasonably available information to identify various possible consideration amounts and considers the probability of the variable consideration for each scenario. The Company’s estimate of transaction price does not include any estimated amount of variable consideration that is constrained.
Significant judgments are required in determining the estimates for each transaction. These estimates include many assumptions, any of which, if incorrect, could result in significant differences between the estimated price and the amount ultimately collected for any given transaction. The Company applies this method consistently to portfolios of similar contracts when estimating the effect of any uncertainty on the amount of variable consideration to which it will be entitled.
In the aggregate, across the numerous transactions within each portfolio, these differences can lead to material variances between estimated and actual revenue in any given period.
The estimate of revenue is necessarily founded on assumptions of payer behavior such as changes in payer mix, payer collections, current customer contractual requirements, and experience with ultimate collection from third-party payers and patients. Each of these aspects of payer behavior (and various others) can change significantly from quarter to quarter, and the Company currently has limited experience with historical payment patterns. Each of these contributes to the potential variability between estimated transaction price and actual consideration received as discussed above, which is expected to be more pronounced early in the process of commercializing a diagnostic test.
The Company makes its best efforts to continually refine its estimates of expected consideration as the Company gains additional experience with collections and historical payment patterns. Accordingly, the Company may update its estimate of the amount of revenue to be recognized for previously delivered tests.
Cost of Revenue
Cost of revenue reflects the aggregate costs incurred in delivering the proteomic testing results to clinicians and includes expenses for third-party specimen collection and shipping costs, as well as the Company’s lab personnel, materials and supplies, equipment and infrastructure expenses associated with clinical testing, and allocated overhead including rent and equipment depreciation. Costs associated with performing the Company’s tests are recorded as the tests are processed regardless of whether and when revenue is recognized with respect to such tests.
Research and Development Expenses
The Company expenses all research and development costs as they are incurred. Research and development expenses consist primarily of personnel costs, stock-based compensation charges, clinical trial costs, and third-party contracted services associated with research and development. The Company recognizes expense associated with third-party contracted services based on the completion of activities as specified in the applicable contracts. Costs incurred under contracts with clinical sites are generally accrued as patient encounters occur, consistent with the terms outlined in the associated contract. Upon termination of contracts with third parties, the Company’s obligations are limited to costs incurred or committed to date. As a result, accrued research and development expenses represent the estimated contractual liability to third parties at the reported period.
Stock-based Compensation
The Company recognizes stock-based compensation for all stock-based awards in accordance with ASC 718, Compensation-Stock Compensation, which requires an entity to measure the cost of employee services received in exchange for an award of equity instruments based on the grant-date fair value of the award.
The fair value of restricted stock units granted under the Company’s equity incentive plans is measured based on the grant-date fair value of the Company’s Class A common stock.
The fair value of stock options granted under the Company’s equity incentive plans is estimated using the Black-Scholes option pricing model. Input assumptions used in calculating the fair value of stock options represent management’s estimates and involve inherent uncertainties and the application of management’s judgment. These input assumptions include the expected term of the awards, the expected common stock price volatility over the term of the awards, risk-free interest rates, and the expected dividend yield.
The fair value of the Company’s Class A common stock is determined by using the closing price per share of the Company’s Class A common stock as reported on Nasdaq. The Company uses the simplified calculation of expected life since the Company does not have sufficient historical exercise data to estimate the expected term. Volatility is based on an average of the historical volatility of the Company’s common stock and the volatilities of the common stock of select comparable publicly-traded entities with characteristics similar to those of the Company. The risk-free rate is based on the U.S. Treasury yield curve in effect at the time of grant for periods corresponding with the expected life of the option. Forfeitures are estimated at the time of grant based on the Company’s historical experience and are adjusted as necessary.
The fair value of equity awards is recognized as compensation cost on a straight-line basis by the Company over the participant’s requisite service period, which is the award’s vesting period. All stock-based compensation costs are
classified in the statements of operations and comprehensive loss based upon the underlying participant’s role within the Company.
Income Taxes
The Company accounts for income taxes under the asset and liability method, which requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the financial statements. Under this method, deferred tax assets and liabilities are determined on the basis of the differences between the financial statement and tax bases of assets and liabilities using enacted tax rates in effect for the year in which the differences are expected to reverse. The effect of a change in tax rates on deferred tax assets and liabilities is recognized in income in the period that includes the enactment date.
The Company recognizes deferred tax assets to the extent that it believes these assets are more likely than not to be realized. In making such a determination, the Company considers all available positive and negative evidence, including future reversals of existing taxable temporary differences, projected future taxable income, tax-planning strategies, and results of recent operations. If the Company determines that it would be able to realize its deferred tax assets in the future in excess of their net recorded amount, the Company would make an adjustment to the deferred tax asset valuation allowance, which would reduce the provision for income taxes.
The Company records uncertain tax positions in accordance with ASC 740 on the basis of a two-step process whereby (1) it determines whether it is more likely than not that the tax positions will be sustained on the basis of the technical merits of the position and (2) for those tax positions that meet the more-likely-than-not recognition threshold, it recognizes the largest amount of tax benefit that is more than 50 percent likely to be realized upon ultimate settlement with the related tax authority.
The Company recognizes interest and penalties related to unrecognized tax benefits within the income tax expense line in the accompanying statements of operations and comprehensive loss. Any accrued interest and penalties related to uncertain tax positions will be reflected as a liability in the balance sheets.
Retirement Savings Plan
The Company sponsors a safe harbor 401(k) plan that covers all of the Company’s eligible employees. The plan allows employees to make contributions up to a specified percentage of their compensation, subject to statutory limitations. The Company makes safe harbor matching contributions equal to 100% of the first 3% of a plan participant’s eligible compensation, plus 50% of the next 2% of a plan participant’s eligible compensation. The Company may also make an additional discretionary match or profit sharing contribution to the plan. The Company recorded expense related to its 401(k) plan of $0.6 million for the years ended December 31, 2023 and 2022.
Segments
The Company operates as one operating segment, which is developing and commercializing its medical diagnostic products and services. The Company’s chief operating decision maker, its chief executive officer, reviews financial information on an aggregate basis for making decisions regarding resource allocation and assessing performance.
Comprehensive Loss
Comprehensive loss consists of net loss and other gains and losses affecting stockholders’ equity that, under U.S. GAAP, are excluded from net loss. For the years ended December 31, 2023 and 2022, comprehensive loss includes unrealized gains (losses) on the Company’s available-for-sale debt securities.
Net Loss per Share
Basic net loss per share is calculated by dividing net loss by the weighted-average number of shares of common stock outstanding for the period, without consideration of potentially dilutive securities. Diluted net loss per share is computed by dividing net loss by the weighted-average number of shares of common stock and potentially dilutive securities outstanding for the period. For purposes of the diluted net loss per share calculation, stock options and warrants to purchase common stock are considered to be potentially dilutive securities. For periods in which the Company reports a net loss, all potentially dilutive shares are anti-dilutive and are therefore excluded from the calculation of diluted net loss per share.
The Company has two classes of common stock and calculates net loss per share using the two-class method. The rights, including the liquidation and dividend rights, of the holders of the Company’s Class A and Class B common stock are identical, except with respect to voting and conversion. The undistributed earnings for each period are allocated based on the contractual participation rights of the Class A and Class B common shares as if the earnings for the period had been distributed. As the liquidation and dividend rights are identical, the undistributed earnings are allocated on a proportionate basis and the resulting amount per share for Class A and Class B common stock was the same for the years ended December 31, 2023 and 2022.
Recently Issued Accounting Pronouncements Not Yet Adopted
In December 2023, the FASB issued ASU 2023-09, Income Taxes (Topic 740): Improvements to Income Tax Disclosures, which is intended to improve the transparency of income tax disclosures by requiring consistent categories and greater disaggregation of information in the effective tax rate reconciliation and income taxes paid by jurisdiction. The ASU is effective for public business entities’ annual periods beginning after December 15, 2024, with early adoption permitted. The Company is currently evaluating the impact of adopting this guidance on its financial statements.
In November 2023, the FASB issued ASU No. 2023-07, Improvements to Reportable Segments Disclosures. While ASU 2023-07 requires incremental disclosures, it does not change how an entity identifies its operating segments, aggregates those operating segments, or applies the quantitative thresholds to determine reportable segments. This ASU is effective for all public business entities for fiscal years beginning after December 15, 2023, and interim periods within fiscal years beginning after December 15, 2024. Entities must adopt the changes to the segment reporting guidance on a retrospective basis. The Company is currently evaluating the impact of adopting this guidance on its financial statements. Early adoption is permitted; however, the Company is not early adopting the standard.
Emerging Growth Company Status
The Company is an emerging growth company, as defined in the Jumpstart Our Business Startups Act of 2012 (the “JOBS Act”). Under the JOBS Act, emerging growth companies can delay adopting new or revised accounting standards until such time as those standards apply to private companies. The Company has elected to use this extended transition period for complying with new or revised accounting standards that have different effective dates for public and private companies until the earlier of the date that it is (a) no longer an emerging growth company or (b) affirmatively and irrevocably opt out of the extended transition period provided in the JOBS Act. As a result, these financial statements may not be comparable to companies that comply with the new or revised accounting pronouncements as of public company effective dates.
3. Cash, Cash Equivalents and Marketable Securities
The Company has classified its marketable securities as available-for-sale. The Company’s cash, cash equivalents and marketable securities by major security type as of December 31, 2023 and 2022 were as follows (in thousands):
| | | | | | | | | | | | | | | | | | | | | | | |
| December 31, 2023 |
| Amortized Cost | | Gross Unrealized Gains | | Gross Unrealized Losses | | Fair Value |
| Cash and cash equivalents: | | | | | | | |
| Cash | $ | 2,608 | | | $ | — | | | $ | — | | | $ | 2,608 | |
| Money market funds | 1,272 | | | — | | | — | | | 1,272 | |
| Total cash and cash equivalents | 3,880 | | | — | | | — | | | 3,880 | |
| Current marketable securities: | | | | | | | |
| Commercial paper | 11,769 | | | 6 | | | (2) | | | 11,773 | |
| Corporate debt securities | 1,155 | | | — | | | (2) | | | 1,153 | |
| U.S. federal agency securities | 19,644 | | | — | | | (102) | | | 19,542 | |
| U.S. government securities | 12,812 | | | — | | | (81) | | | 12,731 | |
| Total current marketable securities | 45,380 | | | 6 | | | (187) | | | 45,199 | |
| Long-term marketable securities: | | | | | | | |
| U.S. federal agency securities | 9,406 | | | 27 | | | (17) | | | 9,416 | |
| U.S. government securities | 4,388 | | | 3 | | | (5) | | | 4,386 | |
| Corporate debt securities | 16,880 | | | 159 | | | — | | | 17,039 | |
| Total long-term marketable securities | 30,674 | | | 189 | | | (22) | | | 30,841 | |
| Total cash, cash equivalents and marketable securities | $ | 79,934 | | | $ | 195 | | | $ | (209) | | | $ | 79,920 | |
| | | | | | | | | | | | | | | | | | | | | | | |
| December 31, 2022 |
| Amortized Cost | | Gross Unrealized Gains | | Gross Unrealized Losses | | Fair Value |
| Cash and cash equivalents: | | | | | | | |
| Cash | $ | 913 | | | $ | — | | | $ | — | | | $ | 913 | |
| Money market funds | 2,618 | | | — | | | — | | | 2,618 | |
| Commercial paper | 26,356 | | | — | | | (9) | | | 26,347 | |
| Total cash and cash equivalents | 29,887 | | | — | | | (9) | | | 29,878 | |
| Current marketable securities: | | | | | | | |
| Commercial paper | 15,219 | | | 2 | | | (66) | | | 15,155 | |
| Corporate debt securities | 507 | | | — | | | (5) | | | 502 | |
| U.S. federal agency securities | 28,964 | | | — | | | (364) | | | 28,600 | |
| U.S. government securities | 8,702 | | | — | | | (133) | | | 8,569 | |
| Total current marketable securities | 53,392 | | | 2 | | | (568) | | | 52,826 | |
| Long-term marketable securities: | | | | | | | |
| U.S. federal agency securities | 9,810 | | | — | | | (199) | | | 9,611 | |
| U.S. government securities | 10,770 | | | — | | | (208) | | | 10,562 | |
| Corporate debt securities | 1,156 | | | — | | | — | | | 1,156 | |
| Total long-term marketable securities | 21,736 | | | — | | | (407) | | | 21,329 | |
| Total cash, cash equivalents and marketable securities | $ | 105,015 | | | $ | 2 | | | $ | (984) | | | $ | 104,033 | |
The following tables summarize the Company’s available-for-sale debt securities and cash equivalents with unrealized losses as of December 31, 2023 and 2022, aggregated by major security type and the length of time that individual securities have been in a continuous loss position (in thousands):
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| December 31, 2023 |
| Less than 12 months | | 12 months or greater | | Total |
| Fair Value | | Unrealized Losses | | Fair Value | | Unrealized Losses | | Fair Value | | Unrealized Losses |
| Commercial paper | $ | 5,453 | | | $ | (2) | | | $ | — | | | $ | — | | | $ | 5,453 | | | $ | (2) | |
| Corporate debt securities | 1,153 | | | (2) | | | — | | | — | | | 1,153 | | | (2) | |
| U.S. federal agency securities | 15,308 | | | (52) | | | 8,751 | | | (67) | | | 24,059 | | | (119) | |
| U.S. government securities | 4,769 | | | (13) | | | 10,895 | | | (73) | | | 15,664 | | | (86) | |
| Total | $ | 26,683 | | | $ | (69) | | | $ | 19,646 | | | $ | (140) | | | $ | 46,329 | | | $ | (209) | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| December 31, 2022 |
| Less than 12 months | | 12 months or greater | | Total |
| Fair Value | | Unrealized Losses | | Fair Value | | Unrealized Losses | | Fair Value | | Unrealized Losses |
| Commercial paper | $ | 40,063 | | | $ | (75) | | | $ | — | | | $ | — | | | $ | 40,063 | | | $ | (75) | |
| Corporate debt securities | 1,156 | | | — | | | 502 | | | (5) | | | 1,658 | | | (5) | |
| U.S. federal agency securities | 12,869 | | | (228) | | | 25,342 | | | (335) | | | 38,211 | | | (563) | |
| U.S. government securities | 10,562 | | | (208) | | | 8,569 | | | (133) | | | 19,131 | | | (341) | |
| Total | $ | 64,650 | | | $ | (511) | | | $ | 34,413 | | | $ | (473) | | | $ | 99,063 | | | $ | (984) | |
As of December 31, 2023 and 2022, the Company had not recorded any allowance for credit losses related to its available-for-sale securities. The Company attributes the declines in the fair value of its available-for-sale securities to normal market and interest rate fluctuations. The declines in fair value are not attributed to declines in credit quality. The Company does not intend to sell investments while they are in an unrealized loss position and does not believe that it is more likely than not that the Company will be required to sell the investments before recovery of their amortized cost basis, which may be maturity. All of the Company’s investments mature in less than two years.
The Company’s marketable securities classified by contractual maturities as of December 31, 2023 were as follows (in thousands):
| | | | | | | | | | | |
| Amortized Cost | | Fair Value |
| Due within one year | $ | 45,380 | | | $ | 45,199 | |
| Due after one year through five years | 30,674 | | | 30,841 | |
| Total | $ | 76,054 | | | $ | 76,040 | |
4. Property and Equipment
The following table presents the components of property and equipment, net, as of December 31, 2023 and 2022 (in thousands):
| | | | | | | | | | | |
| December 31, |
| 2023 | | 2022 |
| Laboratory equipment | $ | 5,734 | | | $ | 5,914 | |
| Computer equipment | 1,054 | | | 1,230 | |
| Leasehold improvements | 772 | | | 710 | |
| Software | 1,141 | | | 1,141 | |
| Furniture and fixtures | 320 | | | 320 | |
| Total property and equipment | 9,021 | | | 9,315 | |
| Less accumulated depreciation and amortization | (7,022) | | | (6,256) | |
| Property and equipment, net | $ | 1,999 | | | $ | 3,059 | |
Depreciation and amortization expense was $0.9 million and $0.8 million for the years ended December 31, 2023 and 2022, respectively.
5. Accrued and Other Current Liabilities
The following table presents the components of accrued and other current liabilities as of December 31, 2023 and 2022 (in thousands):
| | | | | | | | | | | |
| December 31, |
| 2023 | | 2022 |
| Accrued compensation | $ | 779 | | | $ | 2,290 | |
| Accrued vacation | 365 | | | 430 | |
| Accrued 401(k) matching contributions | 74 | | | 568 | |
| Operating lease liability, current portion | 578 | | | 519 | |
| Other current liabilities | 926 | | | 637 | |
| Total accrued and other current liabilities | $ | 2,722 | | | $ | 4,444 | |
6. Other Income, net
The following table presents the components of other income, net, for the years ended December 31, 2023 and 2022 (in thousands):
| | | | | | | | | | | |
| Year Ended
December 31, |
| 2023 | | 2022 |
| Interest income | $ | 1,640 | | | $ | 456 | |
| Investment income, net | 1,994 | | | 1,071 | |
| Other income, net | $ | 3,634 | | | $ | 1,527 | |
7. Fair Value Measurements
As of December 31, 2023 and 2022, the carrying amounts of the Company’s receivables, prepaid and other current assets, accounts payable, and accrued and other current liabilities approximate their fair values, principally due to the short-term nature of the assets and liabilities. The recorded values of the finance leases approximate fair value as the interest rates approximate market interest rates.
Money market funds are highly liquid investments and are actively traded. The pricing information on money market funds is readily available and can be independently validated as of the measurement date. This approach results in the classification of these securities as Level 1 of the fair value hierarchy.
U.S. government agency bonds, U.S. government bonds, commercial paper, and corporate debt securities are measured at fair value using Level 2 inputs. The Company reviews trading activity and pricing for these investments as of each measurement date.
The Company follows a fair value hierarchy that prioritizes the inputs to valuation techniques used to measure fair value. Fair value is defined as an exit price, representing the amount that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants. As such, fair value is a market-based measurement that should be determined based on assumptions that market participants would use in pricing an asset or liability. The three levels of the fair value hierarchy are as follows:
Level 1 inputs are observable, quoted prices (unadjusted) in active markets for identical assets or liabilities that the Company can access at the measurement date.
Level 2 inputs are observable inputs other than quoted prices included in Level 1 that are observable either directly or indirectly or quoted prices in markets that are not active; or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities.
Level 3 inputs are unobservable inputs in which there is little or no market data, which require the Company to develop its own assumptions.
The following table shows the Company’s assets measured at fair value on a recurring basis by level within the fair value hierarchy (in thousands) as of December 31, 2023:
| | | | | | | | | | | | | | | | | |
| Level 1 | | Level 2 | | Level 3 |
| Assets: | | | | | |
| Cash equivalents: | | | | | |
| Money market funds | $ | 1,272 | | | $ | — | | | $ | — | |
| Marketable securities: | | | | | |
| Commercial paper | — | | | 11,773 | | | — | |
| Corporate debt securities | — | | | 18,192 | | | — | |
| U.S. federal agency securities | — | | | 28,958 | | | — | |
| U.S. government securities | — | | | 17,117 | | | — | |
| Total assets | $ | 1,272 | | | $ | 76,040 | | | $ | — | |
The following table shows the Company’s assets and liabilities measured at fair value on a recurring basis by level within the fair value hierarchy (in thousands) as of December 31, 2022:
| | | | | | | | | | | | | | | | | |
| Level 1 | | Level 2 | | Level 3 |
| Assets: | | | | | |
| Cash equivalents: | | | | | |
| Money market funds | $ | 2,618 | | | $ | — | | | $ | — | |
| Commercial paper | — | | | 26,347 | | | — | |
| Marketable securities: | | | | | |
| Commercial paper | — | | | 15,155 | | | — | |
| Corporate debt securities | — | | | 1,658 | | | — | |
| U.S. federal agency securities | — | | | 38,211 | | | — | |
| U.S. government securities | — | | | 19,131 | | | — | |
| Total assets | $ | 2,618 | | | $ | 100,502 | | | $ | — | |
8. Related Party Transactions
In June 2019, the Company entered into a master services agreement with Carelon Research, a subsidiary of Elevance Health, Inc. (“Elevance Health”). This agreement covers a range of research projects, including Carelon Research’s role as a contract research organization for the Prematurity Risk Assessment Combined With Clinical Interventions for Improving Neonatal outcoMEs (“PRIME”) study. The Company paid fees related to this agreement of $4.0 million and $2.2 million for the years ended December 31, 2023 and 2022, respectively, which were recorded in research and development expenses in the Company’s statements of operations and comprehensive loss. In November 2020, the Company entered into a Laboratory Services Agreement with Elevance Health related to the PRIME study. This agreement provides a contracted rate for certain tests performed pursuant to the study. The Company recognized revenues related to this agreement of $61 thousand and $100 thousand for the years ended December 31, 2023 and 2022, respectively.
In February 2021, the Company entered into a commercial collaboration agreement with Elevance Health and its affiliates (the “Commercial Collaboration Agreement”). The Commercial Collaboration Agreement provides defined payment within a defined period for use of the PreTRM test within Elevance Health’s network of covered members. Pursuant to the Commercial Collaboration Agreement, Elevance Health will purchase a certain minimum number of tests for each of the first three years of the term of the agreement. Additionally, Elevance Health agreed to pay a certain minimum amount per year for the first three years of the term of the Commercial Collaboration Agreement. The Company received $6.0 million during the year ended December 31, 2023, which amount related to the minimum payments for the year ended December 31, 2022. As of December 31, 2023, the Company recorded $11.2 million in other receivables related to the minimum payments for the year ended December 31, 2023, which was received in January 2024. Such minimum payments are initially recorded as deferred revenue. Deferred revenue is recognized as revenue when the Company delivers PreTRM test results to Elevance Health patients pursuant to the Commercial Collaboration Agreement. The Company also agreed to develop a sales, marketing, and customer service program, and to provide training and marketing to duly licensed physicians specializing in obstetrics and gynecology or family medicine, or licensed nurse midwives, at the reasonable request of Elevance Health.
Elevance Health has been participating in the Company’s PRIME study and at the conclusion of the PRIME study, under the Commercial Collaboration Agreement, the parties agreed to use commercially reasonable efforts to enter into Elevance Health’s standard lab provider agreement. Unless earlier terminated due to breach, the Commercial Collaboration Agreement will remain in effect until the later of (a) the third anniversary of the effective date or (b) the date on which Elevance Health has purchased a fixed number of PreTRM tests as agreed by the parties.
The Commercial Collaboration Agreement with Elevance Health is considered to be within the scope of ASC Topic 808, Collaborative Arrangements (“ASC 808”), as the parties are active participants and exposed to the risks and rewards of the collaborative activity. The Company determined the PreTRM tests to be a performance obligation for which Elevance Health is a customer and a unit of account within the scope of ASC 606. The associated transaction price is based on the contractual minimum number of tests and the agreed upon defined payment amount per test. The transaction price was allocated to this single performance obligation, which will be recognized upon delivery of test results expected to occur over the term of the agreement. All other items promised to Elevance Health are immaterial in the context of the Commercial Collaboration Agreement. There were no material revenues related to the Commercial Collaboration Agreement for the years ended December 31, 2023 and 2022.
9. Capital Structure
Common Stock
The Company has two authorized classes of common stock, Class A and Class B. The rights of the holders of Class A and Class B common stock are identical, except with respect to voting and conversion. Each share of Class A common stock is entitled to one vote and shares of Class B common stock are non-voting. Each share of Class B common stock may be converted at any time to one share of Class A common stock at the option of its holder, subject to the ownership limitations provided for in the Company’s amended and restated certificate of incorporation. In September 2023, holders of Class B common stock converted 437,500 shares of Class B common stock to 437,500 shares of Class A common stock.
The following shares of Class A common stock were reserved for future issuance:
| | | | | | | | | | | |
| December 31, |
| 2023 | | 2022 |
| Warrants to purchase Class A common stock | 2,775,978 | | | 2,775,978 | |
| Options to purchase Class A common stock | 7,251,663 | | | 8,428,441 | |
| Restricted stock units outstanding | 2,692,459 | | | — | |
| Class A common stock available for future grants under the 2021 Equity Incentive Plan | 1,002,091 | | | 1,926,356 | |
| Class A common stock available for future grants under the 2021 Employee Stock Purchase Plan | 801,668 | | | 598,777 | |
| Total | 14,523,859 | | | 13,729,552 | |
Preferred Stock
The Company is authorized to issue up to 5,000,000 shares of preferred stock, par value $0.0001 per share. There were no preferred shares outstanding at December 31, 2023 and 2022.
10. Stock-Based Compensation
Equity Incentive Plans
In November 2011, the Company established the 2011 Employee, Director and Consultant Equity Incentive Plan (the “2011 Plan”) and reserved shares of the Company’s common stock for sale and issuance under the 2011 Plan. Options granted under the 2011 Plan generally vest over a four-year period and generally expire ten years from the date of grant. Options are exercisable only to the extent vested. The 2011 Plan terminated in November 2021, and accordingly, no additional shares are available for grant under the 2011 Plan. The 2011 Plan continues to govern outstanding awards granted under the 2011 Plan.
The 2021 Equity Incentive Plan (the “2021 Plan”) was established in July 2021. The 2021 Plan provides for the grant of incentive and non-statutory stock options as well as other stock rights to employees, directors and consultants of the Company. Options generally vest over a four-year period, are exercisable only to the extent vested, and generally expire ten years from the date of grant. Restricted stock units (“RSUs”) generally vest over either a two-year or four-year period. The 2021 Plan includes provisions for annual automatic increases to the number of shares of Class A common stock reserved for issuance under the 2021 Plan. In addition, any shares that otherwise would be returned to the 2011 Plan as a result of the expiration or cancellation of stock options may be added to the 2021 Plan. As of December 31, 2023, there were 1,002,091 shares of the Company’s Class A common stock that were available for future grants under the 2021 Plan.
The 2021 Employee Stock Purchase Plan (the “2021 ESPP”) was established in July 2021. The 2021 ESPP includes provisions for annual automatic increases to the number of shares of Class A common stock reserved for issuance under the 2021 ESPP. As of December 31, 2023, there were 801,668 shares of the Company’s Class A common stock that were available for future grants under the 2021 ESPP.
Stock Options
Unless otherwise noted, references to “options” in the subsequent disclosures, refers to the combined incentive and non-statutory stock options issued as employee and non-employee stock-based compensation, and authorized under the 2011 Plan and the 2021 Plan. The following table summarizes information about these options granted and outstanding:
| | | | | | | | | | | | | | | | | | | | | | | |
| Number of
Shares
Subject to
Options
Outstanding | | Weighted-
Average
Exercise Price
Per Share | | Weighted-
Average
Remaining
Contractual
Life (In Years) | | Aggregate Intrinsic Value (In Thousands) |
| Outstanding — December 31, 2022 | 8,428,441 | | | $ | 3.65 | | | 7.7 | | $ | 115 | |
| Granted | 991,866 | | | 3.49 | | | | | |
| Expired | (14,430) | | | 0.75 | | | | | |
| Cancelled | (1,561,123) | | | 4.25 | | | | | |
| Exercised | (593,091) | | | 1.85 | | | | | |
| Outstanding — December 31, 2023 | 7,251,663 | | | $ | 3.66 | | | 6.9 | | $ | 20,014 | |
| Vested and expected to vest at December 31, 2023 | 7,120,916 | | | $ | 3.64 | | | 6.9 | | $ | 19,763 | |
| Vested and exercisable at December 31, 2023 | 5,477,835 | | | $ | 3.28 | | | 6.5 | | $ | 16,856 | |
The weighted-average grant date fair value of options granted during the years ended December 31, 2023 and 2022 was $2.28 and $1.92 per share, respectively. The total aggregate intrinsic value of options exercised during the years ended December 31, 2023 and 2022 was $1.4 million and $0.5 million, respectively. The total fair value of options vested for the years ended December 31, 2023 and 2022 was $4.8 million and $5.8 million, respectively.
The fair values calculated using the Black-Scholes option pricing model were estimated on each grant date using the following assumptions:
| | | | | | | | | | | |
| Year Ended December 31, |
| 2023 | | 2022 |
| Expected volatility | 70.1% - 72.4% | | 63.7% - 69.1% |
| Risk-free interest rate | 3.7% - 4.2% | | 1.7% - 4.3% |
| Expected term (in years) | 5.3 - 7.0 | | 5.3 - 7.0 |
| Expected dividend yield | — | % | | — | % |
RSUs
The following table summarizes information about RSUs granted and outstanding under the 2021 Plan:
| | | | | | | | | | | |
| Number of Awards | | Weighted-Average Grant Date Fair Value |
| Outstanding — December 31, 2022 | — | | | $ | — | |
| Granted | 2,827,824 | | | 2.10 | |
| Forfeited | (135,365) | | | 3.76 | |
| Vested | — | | | — | |
| Outstanding — December 31, 2023 | 2,692,459 | | | $ | 2.01 | |
Stock-Based Compensation Expense
The following table presents the impact of stock-based compensation expense in the statements of operations for the periods indicated (in thousands):
| | | | | | | | | | | |
| Year Ended
December 31, |
| 2023 | | 2022 |
| Research and development expense | $ | 1,574 | | | $ | 1,671 | |
| Sales and marketing expense | 657 | | | 590 | |
| General and administrative expense | 3,042 | | | 2,794 | |
| Total employee stock-based compensation | $ | 5,273 | | | $ | 5,055 | |
The information about unrecognized stock-based compensation expense for outstanding unvested stock options and RSUs as of December 31, 2023 was as follows (in thousands, except years):
| | | | | | | | | | | |
| Unrecognized Stock-Based Compensation Expense | | Weighted-Average Period of Recognition (in years) |
| Stock Options | $ | 5,035 | | | 1.6 |
| RSUs | 3,942 | | | 2.7 |
| Total unrecognized stock-based compensation expense | $ | 8,977 | | | |
11. Warrants
All outstanding common stock warrants were exercisable immediately when granted. All outstanding common stock warrants are exercisable for shares of Class A common stock. The Company’s common stock warrants outstanding were as follows:
| | | | | | | | | | | | | | |
| | Number of Warrants Outstanding as of: |
| Exercise Price | | December 31, 2023 | | December 31, 2022 |
| $ | 5.20 | | | 3,473 | | | 3,473 | |
| 9.03 | | | 1,032,404 | | | 1,032,404 | |
| 10.84 | | | 1,009,795 | | | 1,009,795 | |
| 12.38 | | | 8,083 | | | 8,083 | |
| 20.77 | | | 722,223 | | | 722,223 | |
| | 2,775,978 | | | 2,775,978 | |
12. Commitments and Contingencies
Leases
The Company is the lessee in all of its lease arrangements. The Company did not enter into any leases with related parties during the presented periods. The Company makes assumptions and judgments when assessing contracts for lease components, determining lease classifications, and calculating right-of-use asset and lease liability values. These assumptions and judgments may include the useful lives and fair values of the leased assets, the implicit rate underlying the Company’s leases, the Company’s incremental borrowing rate or the Company’s intent to exercise or not exercise options available in lease contracts.
The following table shows right-of-use assets and lease liabilities, and the associated financial statement line items as of December 31, 2023 and 2022 (in thousands):
| | | | | | | | | | | | | | | | | | | | |
| | | | December 31, |
| Lease-Related Assets and Liabilities | | Financial Statement Line Items | | 2023 | | 2022 |
| Right-of-use assets: | | | | | | |
| Operating leases | | Other assets | | $ | 1,180 | | | $ | 1,707 | |
| Finance leases | | Property and equipment, net | | 1,008 | | | 1,317 | |
| Total right-of-use assets | | | | $ | 2,188 | | | $ | 3,024 | |
| | | | | | |
| Lease liabilities: | | | | | | |
| Operating leases | | Accrued and other current liabilities | | $ | 578 | | | $ | 519 | |
| | Operating lease obligation, net of current portion | | 644 | | | 1,222 | |
| Finance leases | | Finance lease obligation, current portion | | 440 | | | 464 | |
| | Finance lease obligation, net of current portion | | 196 | | | 626 | |
| Total lease liabilities | | | | $ | 1,858 | | | $ | 2,831 | |
Lease costs and other information consisted of the following (in thousands, except terms and rates):
| | | | | | | | | | | | | | |
| | Year Ended December 31, |
| | 2023 | | 2022 |
| Lease cost | | | | |
| Finance lease cost: | | | | |
| Amortization of right-of-use assets | | $ | 312 | | | $ | 280 | |
| Interest on lease liabilities | | 55 | | | 61 | |
| Operating lease cost | | 636 | | | 504 | |
| Total lease cost | | $ | 1,003 | | | $ | 845 | |
| | | | |
| Other information | | | | |
| Finance leases: | | | | |
| Operating cash outflows | | $ | 55 | | | $ | 48 | |
| Financing cash outflows | | $ | 466 | | | $ | 303 | |
| Right-of-use assets obtained in exchange for lease liabilities | | $ | 18 | | | $ | 1,253 | |
| Weighted-average remaining lease term (in years) | | 1.4 | | 2.3 |
| Weighted-average discount rate | | 6.5% | | 6.4% |
| Operating leases: | | | | |
| Operating cash outflows | | $ | 628 | | | $ | 609 | |
| Right-of-use assets obtained in exchange for lease liabilities | | $ | — | | | $ | 2,169 | |
| Weighted-average remaining lease term (in years) | | 2.0 | | 3.0 |
| Weighted-average discount rate | | 7.5% | | 7.5% |
Future minimum lease payments for the Company’s leases as of December 31, 2023 were as follows (in thousands):
| | | | | | | | | | | | | | | | | | | | |
| | Operating Leases | | Finance Leases | | Total |
| 2024 | | $ | 646 | | | $ | 467 | | | $ | 1,113 | |
| 2025 | | 666 | | | 197 | | | 863 | |
| 2026 | | — | | | 2 | | | 2 | |
| 2027 and thereafter | | — | | | — | | | — | |
| Total minimum lease payments | | 1,312 | | | 666 | | | 1,978 | |
| Less: imputed interest | | (90) | | | (30) | | | (120) | |
| Present value of future lease payments | | 1,222 | | | 636 | | | 1,858 | |
| Less: current portion | | 578 | | | 440 | | | 1,018 | |
| Long-term portion | | $ | 644 | | | $ | 196 | | | $ | 840 | |
Operating Leases
The Company leases a total of approximately 24,300 square feet of office and laboratory space under a single non-cancelable operating lease with a termination date of December 31, 2025 (as amended, the “Office Lease”). The Office Lease includes an early termination right which termination would occur under certain circumstances, as provided in the amended Office Lease, after July 1, 2024 if exercised. The Company is not currently reasonably certain it will exercise the termination right. The implicit rate provided in the Company’s operating lease is not readily determinable. As such, the Company uses its incremental borrowing rate to calculate the present value of its operating lease liabilities.
Finance Leases
The Company leases certain equipment related to its information technology infrastructure and laboratory operations. All of the Company’s current finance leases include bargain purchase options that the Company is reasonably certain to exercise. The Company has elected not to separate lease and non-lease components for its equipment leases. The rates implicit in the Company’s finance leases are determinable, and the Company uses those rates to calculate the present value of its finance lease liabilities.
Indemnification
The Company has agreed to indemnify its officers and directors for certain events or occurrences, while the officer or director is or was serving at the Company’s request in such capacity. The maximum amount of potential future indemnification is unlimited; however, the Company purchases director and officer insurance coverage that provides for corporate reimbursements of covered obligations that limits the Company’s exposure and enables it to recover a portion of potential future amounts paid. The Company is unable to reasonably estimate the maximum amount that could be payable under these arrangements since these obligations are not capped but are conditional to the unique facts and circumstances involved. Accordingly, the Company has no liabilities recorded for these agreements as of December 31, 2023 and 2022. The Company has never incurred costs to defend lawsuits or settle claims related to these indemnification agreements.
Employee Agreements
The Company has signed various employment agreements with key executives pursuant to which if their employment is terminated by the Company without cause or by the employees for good reason, or following a change of control of the Company, the employees are entitled to receive certain benefits, including severance payments, accelerated vesting of stock and stock options, and certain insurance benefits.
Legal Matters
The Company is not currently a party to any material litigation or other material legal proceedings. The Company may, from time to time, be involved in various legal proceedings arising from the normal course of business activities, and an unfavorable resolution of any of these matters could materially affect the Company’s future results of operations, cash flows, or financial position.
13. Income Taxes
The Company has not recorded any income tax expense for the years ended December 31, 2023 and 2022 due to its history of operating losses.
The provision for income taxes includes the following components for the years ended December 31, 2023 and 2022 (in thousands):
| | | | | | | | | | | |
| Year Ended
December 31, |
| 2023 | | 2022 |
| Current: | | | |
| Federal | $ | — | | $ | — |
| State | — | | — |
| Total current benefit (provision) | $ | — | | $ | — |
| Deferred: | | | |
| Federal | $ | 8,178 | | $ | 9,400 |
| State | 2,198 | | 1,951 |
| Change in valuation allowance | (10,376) | | (11,351) |
| Total deferred benefit (provision) | $ | — | | $ | — |
| Total income tax benefit (provision) | $ | — | | $ | — |
The benefit (provision) for income taxes differs from the amount computed at federal statutory rates as follows (in thousands):
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2023 | | 2022 |
| Computed Federal income tax benefit (expense) at the statutory rate | $ | 7,602 | | | 21.00 | % | | $ | 9,278 | | | 21.00 | % |
| R&D credits | 698 | | | 1.93 | % | | 566 | | | 1.28 | % |
| Equity-based expenses | (63) | | | (0.17) | % | | (325) | | | (0.74) | % |
| State income taxes, net of federal benefit | 1,783 | | | 4.92 | % | | 1,771 | | | 4.01 | % |
| State net operating loss carryforward true up | 154 | | | 0.42 | % | | (8) | | | (0.02) | % |
| Change in statutory rates | 163 | | | 0.45 | % | | 78 | | | 0.18 | % |
| Other | 39 | | | 0.11 | % | | (9) | | | (0.02) | % |
| Valuation allowance | (10,376) | | | (28.66) | % | | (11,351) | | | (25.69) | % |
| Income tax benefit (provision) | $ | — | | | — | % | | $ | — | | | — | % |
Significant components of the Company’s net deferred income tax assets (liabilities) are as follows (in thousands):
| | | | | | | | | | | |
| December 31, |
| 2023 | | 2022 |
| Deferred tax assets: | | | |
| Net operating loss carryforwards | $ | 53,072 | | $ | 46,674 |
| R&D credits | 3,856 | | 3,038 |
| R&E expenses | 5,219 | | 2,644 |
| Accruals and reserves | 278 | | 635 |
| Equity-based compensation | 2,440 | | 1,496 |
| Depreciation and amortization | — | | 5 |
| Lease liability | 317 | | 438 |
| Other | 7 | | 3 |
| Total deferred tax asset before allowance | 65,189 | | 54,933 |
| Less: valuation allowance | (64,879) | | (54,504) |
| Total deferred tax asset | 310 | | 429 |
| Deferred tax liabilities: | | | |
| Right-of-use asset | (306) | | (429) |
| Depreciation and amortization | (4) | | — |
| Net deferred tax assets | $ | — | | $ | — |
Management assesses the available positive and negative evidence to estimate if sufficient future taxable income will be generated to use the existing deferred tax assets. A significant piece of objective negative evidence evaluated is the cumulative loss incurred since inception. Such objective evidence limits the ability to consider other subjective evidence such as the Company’s projections for future growth.
On the basis of this evaluation, a full valuation allowance of $64.9 million and $54.5 million has been recorded as of December 31, 2023 and 2022, respectively, as it is more likely than not that the deferred tax assets will not be realized. The valuation allowance increased by $10.4 million and $11.4 million for the years ended December 31, 2023 and 2022, respectively, and there is no tax benefit presented in the accompanying financial statements.
The Company is subject to minimum taxes in several of the state jurisdictions where it files income tax returns. The amounts paid are immaterial and not presented above as a component of the current state tax provision.
As of December 31, 2023, the Company had U.S. federal and state net operating loss carryforwards of approximately $211.6 million and $143.7 million, respectively. Of the federal amount, $141.3 million can be carried forward indefinitely, while the remainder begins to expire after 2028, if not utilized. The state amounts begin to expire at various dates after 2030.
Because of the change of ownership provisions of the Tax Reform Act of 1986, use of a portion of the Company’s NOL and tax credit carryforwards may be limited in future periods. Further, a portion of the carryforwards may expire before being applied to reduce future income tax liabilities. There are currently no federal or state tax audits in progress. All prior tax years remain subject to examination by Federal and State of Utah authorities due to the existence of net operating loss carryforwards.
The Company recognizes the tax benefit of an uncertain tax position only if it is more likely than not that a tax position will be sustained upon examination by the appropriate taxing authorities, based on technical merits. The reversal of the uncertain tax positions would not affect the Company’s effective tax rate to the extent that it continues to maintain a full valuation allowance against its deferred tax assets. As of December 31, 2023 and 2022, the Company did not record any material interest expense or penalties related to uncertain tax positions or the settlement of audits for prior periods. The
Company does not expect a significant increase or decrease in its uncertain tax positions within the next 12 months. A reconciliation of the beginning and ending amount of uncertain tax positions (in thousands):
| | | | | | | | | | | |
| Year Ended
December 31, |
| 2023 | | 2022 |
| Balance at the beginning of the year | $ | 2,025 | | | $ | 1,648 |
| Gross increases—prior period | 80 | | | — |
| Gross increases—current period | 465 | | | 377 |
| Balance at the end of the year | $ | 2,570 | | | $ | 2,025 |
14. Net loss per share
The Company calculates net loss per share of Class A and Class B common stock using the two-class method. For periods in which the Company reports a net loss, all potentially dilutive shares are anti-dilutive and are therefore excluded from the calculation of diluted net loss per share. For the years ended December 31, 2023 and 2022, the Company reported net losses and as such, basic and diluted net loss per share are the same.
As the liquidation and dividend rights are identical for Class A and Class B common shares, the undistributed earnings are allocated on a proportionate basis and the resulting amount per share for Class A and Class B common stock was the same for the years ended December 31, 2023 and 2022.
The Company excluded the following potentially dilutive securities, presented based on amounts outstanding at each period end, from the computation of diluted net loss per share for the periods indicated because their impact would have been anti-dilutive:
| | | | | | | | | | | |
| December 31, |
| 2023 | | 2022 |
| Warrants to purchase Class A common stock | 2,775,978 | | | 2,775,978 | |
| Options to purchase Class A common stock | 7,251,663 | | | 8,428,441 | |
| Restricted stock units outstanding | 2,692,459 | | | — | |
| Total | 12,720,100 | | | 11,204,419 | |
Item 9. Changes in and Disagreements With Accountants on Accounting and Financial Disclosure
None.
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
We maintain “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act, that are designed to ensure that information required to be disclosed in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed in the reports that we file or submit under the Exchange Act is accumulated and communicated to our management, including our principal executive and principal financial officers, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure. Our management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and our management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures.
Our management, with the participation of our Chief Executive Officer (our principal executive officer) and Chief Financial Officer (our principal financial officer and principal accounting officer), evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2023. Based on the evaluation of our disclosure controls and
procedures as of December 31, 2023, our Chief Executive Officer and Chief Financial Officer concluded that, as of such date, our disclosure controls and procedures were effective at the reasonable assurance level.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting that occurred during the period covered by this Annual Report on Form 10-K that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act. Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management assessed the effectiveness of our internal control over financial reporting as of December 31, 2023. In making this assessment, management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control-Integrated Framework. Based on our assessment, management believes that, as of December 31, 2023, our internal control over financial reporting is effective based on those criteria.
Item 9B. Other Information
Rule 10b5-1 Trading Arrangements
On December 15, 2023, John J. Boniface, Ph.D., our Chief Scientific Officer, adopted a Rule 10b5-1 trading arrangement that is intended to satisfy the affirmative defense of Rule 10b5-1(c) for the sale of 120,737 shares.
None of the other officers (as defined in Section 16 of the Securities Exchange Act of 1934, as amended) and directors adopted or terminated any contract, instruction, or written plan for the purchase or sale of our securities that was intended to satisfy the affirmative defense of Rule 10b5-1(c) or any “non-Rule 10b5-1 trading arrangement,” as defined in Item 408(a) of Regulation S-K.
Equity Award Modifications
As previously reported, effective June 8, 2023, Zhenya Lindgardt, a member of the Board, was appointed as the interim Chief Executive Officer of the Company, concurrently with the retirement of Gregory C. Critchfield, M.D., M.S., former President and Chief Executive Officer of the Company and former Chairman of the Board. On November 6, 2023, Ms. Lindgardt was granted 800,000 restricted stock units, to vest in equal quarterly installments over four years, beginning on February 6, 2024, subject to Ms. Lindgardt’s continued employment with the Company on the relevant vesting date (the “2023 Lindgardt RSUs”).
On March 15, 2024, the Board approved the acceleration of the vesting of 100,000 of the 2023 Lindgardt RSUs, effective as of March 23, 2024, to better align the vesting of the 2023 Lindgardt RSUs with the commencement of Ms. Lindgardt’s services as interim Chief Executive Officer. The remaining unvested 2023 Lindgardt RSUs will continue to vest in 13 quarterly installments beginning on June 8, 2024.
Also, as previously reported, effective June 7, 2023, Austin Aerts, the Company’s former Vice President of Finance and Corporate Controller, was appointed as the interim Chief Financial Officer of the Company, concurrently with the resignation of Jay Moyes, former Treasurer and Chief Financial Officer of the Company. On November 6, 2023, Mr. Aerts was granted 210,000 restricted stock units, to vest in equal quarterly installments over four years, beginning on February 6, 2024, subject to Mr. Aerts’s continued employment with the Company on the relevant vesting date (the “2023 Aerts RSUs”).
On March 15, 2024, the Board approved the acceleration of the vesting of 26,250 of the 2023 Aerts RSUs effective as of March 22, 2024, to better align the vesting of the 2023 Aerts RSUs with the commencement of Mr. Aerts’s services as
interim Chief Financial Officer. The remaining unvested 2023 Aerts RSUs will continue to vest in 13 quarterly installments beginning on June 7, 2024.
Item 9C. Disclosure Regarding Foreign Jurisdiction that Prevent Inspections
Not applicable.
PART III
Item 10. Directors, Executive Officers and Corporate Governance
The response to this item is incorporated by reference from the discussion responsive thereto under the captions “Board of Directors and Corporate Governance” and “Executive Officers” in our Proxy Statement to be filed with the SEC within 120 days of the fiscal year ended December 31, 2023 in connection with the solicitation of proxies for our 2024 annual meeting of stockholders.
Item 11. Executive Compensation
The response to this item is incorporated by reference from the discussion responsive thereto under the captions “Non-Employee Director Compensation” and “Executive Compensation” in our Proxy Statement to be filed with the SEC within 120 days of the fiscal year ended December 31, 2023.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The response to this item is incorporated by reference from the discussion responsive thereto under the caption “Security Ownership of Certain Beneficial Owners and Management” in our Proxy Statement to be filed with the SEC within 120 days of the fiscal year ended December 31, 2023.
Item 13. Certain Relationships and Related Transactions, and Director Independence
The response to this item is incorporated by reference from the discussion responsive thereto under the captions “Certain Relationships, Related Party and Other Transactions” and “Board of Directors and Corporate Governance” in our Proxy Statement to be filed with the SEC within 120 days of the fiscal year ended December 31, 2023.
Item 14. Principal Accounting Fees and Services
The response to this item is incorporated by reference from the discussion responsive thereto under the caption “Ratification of Appointment of Independent Registered Public Accounting Firm” in our Proxy Statement to be filed with the SEC within 120 days of the fiscal year ended December 31, 2023.
PART IV
Item 15. Exhibit and Financial Statement Schedules
(a) Documents filed as part of this report
(1) Financial Statements
See “Index to Financial Statements” at Item 8 to this Annual Report on Form 10-K.
(2) Financial Statement Schedules
Financial statement schedules have been omitted because they are not applicable or because the required information is included in the financial statements and accompanying notes included in this Form 10-K.
(3) Exhibits
| | | | | | | | |
Exhibit Number | | Description |
| 3.1 | | |
| 3.2 | | |
| 3.3 | | |
| 4.1 | | |
| 4.2 | | |
| 4.3 | | |
| 4.4 | | |
| 4.5 | | |
| 4.6 | | |
| 10.1 | | |
| 10.2+ | | |
| 10.3+ | | |
| 10.4*+ | | |
| 10.5† | | |
| 10.6† | | |
| | | | | | | | |
| 10.7† | | |
| 10.7.1† | | |
| 10.7.2*† | | |
| 10.8+ | | |
| 10.9+ | | |
| 10.10+ | | |
| 10.11+ | | |
| 10.12+ | | |
| 10.13*+ | | |
| 10.14+ | | |
| 10.15+ | | |
| 10.16*+ | | |
| 10.17+ | | |
| 10.18*+ | | |
| 10.19+ | | |
| 10.20+ | | |
| 10.21+ | | |
| 10.22+ | | |
| 10.23*+ | | |
| | | | | | | | |
| 10.24+ | | |
| 10.25+ | | |
| 10.26+ | | |
| 10.27+ | | |
| 10.28*+ | | |
| 10.29*+ | | |
| 10.30 | | |
| 10.31 | | |
| 10.32 | | |
| 10.33 | | |
| 21.1 | | |
| 23.1* | | |
| 24.1* | | |
| 31.1* | | |
| 31.2* | | |
| 32.1** | | |
| 97.1* | | |
| 101.INS | | Inline XBRL Instance Document – the instance document does not appear in the Interactive Data File because XBRL tags are embedded within the Inline XBRL document. |
| 101.SCH | | Inline XBRL Taxonomy Extension Schema Document |
| 101.CAL | | Inline XBRL Taxonomy Extension Calculation Linkbase Document |
| 101.DEF | | Inline XBRL Taxonomy Extension Definition Linkbase Document |
| 101.LAB | | Inline XBRL Taxonomy Extension Label Linkbase Document |
| 101.PRE | | Inline XBRL Taxonomy Extension Presentation Linkbase Document |
| 104 | | Cover Page Interactive Data File (embedded within the Inline XBRL document) |
__________________________________
* Filed herewith.
** The Certification attached as Exhibit 32.1 that accompanies this Annual Report on Form 10-K is not deemed filed with the Securities and Exchange Commission and is not to be incorporated by reference into any filing of Sera Prognostics, Inc. under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended,
whether made before or after the date of this Form 10-K, irrespective of any general incorporation language contained in such filing.
+ Indicates a management contract or any compensatory plan, contract or arrangement.
† Portions of this exhibit (indicated by asterisks) have been omitted in accordance with the rules of the Securities and Exchange Commission.
Item 16. Form 10-K Summary
None.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| | | | | |
| SERA PROGNOSTICS, INC. |
| |
| Date: March 20, 2024 | /s/ Zhenya Lindgardt |
| Zhenya Lindgardt |
| President and Chief Executive Officer |
Each person whose individual signature appears below hereby authorizes and appoints Zhenya Lindgardt and Austin Aerts, and each of them, with full power of substitution and resubstitution and full power to act without the other, as his or her true and lawful attorney-in-fact and agent to act in his or her name, place and stead and to execute in the name and on behalf of each person, individually and in each capacity stated below, and to file any and all amendments to this annual report on Form 10-K and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing, ratifying and confirming all that said attorneys-in-fact and agents or any of them or their or his substitute or substitutes may lawfully do or cause to be done by virtue thereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, this report has been signed below by the following persons on behalf of the registrant in the capacities and on the dates indicated.
| | | | | | | | | | | | | | |
| Name | | Title | | Date |
| | | | |
| /s/ Zhenya Lindgardt | | President and Chief Executive Officer (Principal Executive Officer) | | March 20, 2024 |
| Zhenya Lindgardt | | | |
| | | | |
| /s/ Austin Aerts | | Chief Financial Officer (Principal Accounting Officer and Principal Financial Officer) | | March 20, 2024 |
| Austin Aerts | | | |
| | | | |
| /s/ Kim Kamdar, Ph.D. | | Chair of the Board of Directors | | March 20, 2024 |
| Kim Kamdar, Ph.D. | | | | |
| | | | |
| /s/ Jane F. Barlow, M.D. | | Director | | March 20, 2024 |
| Jane F. Barlow, M.D. | | | | |
| | | | |
| /s/ Gregory C. Critchfield, M.D., M.S. | | Director | | March 20, 2024 |
| Gregory C. Critchfield, M.D., M.S. | | | | |
| | | | |
| /s/ Sandra A.J. Lawrence | | Director | | March 20, 2024 |
| Sandra A.J. Lawrence | | | | |
| | | | |
| /s/ Mansoor Raza Mirza, M.D. | | Director | | March 20, 2024 |
| Mansoor Raza Mirza, M.D. | | | | |
| | | | |
| /s/ Joshua Phillips | | Director | | March 20, 2024 |
| Joshua Phillips | | | | |
| | | | |
| /s/ Ryan Trimble | | Director | | March 20, 2024 |
| Ryan Trimble | | | | |
| | | | |
| /s/ Marcus Wilson, Pharm.D. | | Director | | March 20, 2024 |
| Marcus Wilson, Pharm.D. | | | | |